
Ceramic restorations debond. Composite repairs fail at the interface. When a chairside technician skips silane treatment — or uses a degraded primer that sat open on the bench for six months — the adhesive never properly wets the silica-based surface, and the restoration fails in months instead of years. Rework costs time, materials, and patient trust. The fix is not complicated, but it is chemistry-specific: silane coupling agents bridge the otherwise incompatible worlds of inorganic ceramic and organic resin matrix.
Silane coupling agents in dentistry work by chemically bonding to both the silica-based ceramic surface and the organic resin. The most widely used monomer is 3-methacryloxypropyltrimethoxysilane (MPS, CAS 2530-85-0), applied as a 0.5–5 wt% solution in ethanol/water at pH 4–5. Correct application can raise shear bond strength from roughly 5 MPa on untreated feldspathic porcelain to 20 MPa or higher — a difference that separates a durable restoration from an early failure.
What most practitioners and procurement managers underestimate is how much the outcome depends on variables that happen before the silane ever touches a surface — solution pH, hydrolysis time, substrate preparation, and whether the chemistry was formulated for the specific ceramic type in question. A silane primer optimized for feldspathic porcelain does not behave identically on zirconia, and confusing the two is one of the most common sources of unexplained clinical failures in ceramic bonding protocols.
[Silane Coupling Agent](https://siliconchemicals.com/silane-coupling-agents/) Types Used in Dentistry: MPS, Bis-SIMA, and Specialty Grades
3-Methacryloxypropyltrimethoxysilane (MPS/MEMO): The Workhorse Chemistry
MPS — CAS 2530-85-0, also labeled MEMO or γ-MPS depending on supplier — accounts for the large majority of dental silane primers in clinical and laboratory use. Understanding why requires following the molecule through its actual working sequence rather than treating it as a black-box adhesion promoter.
In the bottle, MPS is mixed at 1–2 wt% into 95% ethanol, then acidified with dilute acetic acid to pH 4–5. At that pH and moisture level, the three methoxy groups hydrolyze to silanols (-Si(OH)₃) within minutes. Those silanols are the reactive end: they condense onto surface silanol groups (-Si-OH) present on silica-based ceramics — feldspathic porcelain, lithium disilicate, leucite-reinforced glass — forming covalent Si-O-Si bonds that are stable under wet oral conditions. Meanwhile, the methacrylate tail at the opposite end of the propyl spacer co-polymerizes directly into the BisGMA or TEGDMA resin matrix during light-cure. The molecule is not merely a glue; it creates a genuine covalent bridge across what is otherwise a thermodynamically incompatible ceramic-polymer interface.
Shear bond strength on feldspathic porcelain without silane treatment typically falls in the 4–8 MPa range. With proper MPS priming and HF etching, the same interface reaches 18–30 MPa, depending on etching time, application protocol, and resin system used. That is not a marginal gain — it is the difference between an acceptable restoration and one that debonds within the first thermal cycling events.
Bis-SIMA, APTES, and Metal-Oxide Primers
Bis-[3-(triethoxysilyl)propyl]-tetrasulfide (TESPT, sometimes called Bis-SIMA in dental literature) and 3-aminopropyltriethoxysilane (APTES) appear primarily in experimental adhesive systems and in primers designed for metal oxide substrates — alumina-blasted zirconia, alumina copings, or metal alloy surfaces after sandblasting.
APTES works through a different mechanism: the primary amine group reacts with aldehyde or epoxy groups in certain resin formulations, or forms ionic interactions with acid-modified resin monomers, rather than direct methacrylate co-polymerization. On alumina-blasted base-metal alloys, APTES-based primers show measurable bond improvement, though the bond mode is less durable under hydrolytic fatigue than MPS on silica ceramics. For production formulators, APTES is a viable secondary coupling agent in multi-component systems, not a drop-in MPS replacement.
Single-Component vs. Two-Bottle Systems: Stability Is the Hidden Variable
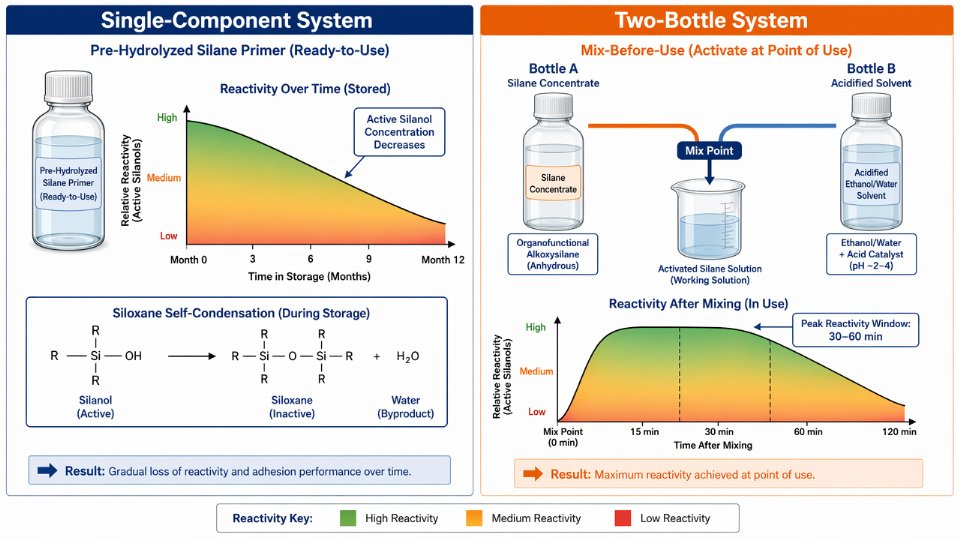
Pre-hydrolyzed, single-component silane primers — common in chairside dental kits — are formulated for convenience. The silanols are already generated. The trade-off is shelf life: pre-hydrolyzed silane solutions undergo gradual self-condensation (silanol + silanol → siloxane + water), reducing active monomer concentration over 6–12 months even under refrigeration. A bottle used at month eleven has measurably less reactive silane than one used at month two.
Two-bottle systems, where the silane concentrate and the acidified solvent are mixed immediately before use, sidestep this problem. Reactivity is at its peak for roughly 30–60 minutes post-mixing. For high-volume laboratory workflows or clinical situations where bonding reliability is non-negotiable, two-bottle formats are worth the added preparation step.
Pre-hydrolyzed single-component dental silane primers have a shorter effective shelf life than two-bottle systems requiring chairside mixingTrue
Pre-hydrolyzed silanes contain active silanols that gradually self-condense into inactive oligomers during storage, reducing bonding efficacy over time. Two-bottle systems generate fresh silanols only at point of use, preserving full reactivity.
Zirconia: Where MPS Alone Falls Short
Pure zirconia (ZrO₂) presents a practical problem MPS cannot solve on its own. The surface carries zirconium hydroxide groups (Zr-OH), not silicon-based silanols — so the Si-O-Si condensation pathway that works on glass ceramics simply does not apply at useful rates. Bond strengths with MPS-only primers on unmodified zirconia typically stay below 10 MPa, well under clinical reliability thresholds.
Two strategies show clinical and laboratory evidence of improvement. The first combines MPS with 10-MDP (10-methacryloyloxydecyl dihydrogen phosphate), where the phosphate group forms a chemical bond with zirconium oxide directly while the methacrylate end integrates with resin. Bond strengths with MDP-containing zirconia primers range from 15–35 MPa depending on surface pre-treatment and thermal aging conditions. The second approach uses sulfonate-functional silanes, which interact with basic zirconia surface sites through acid-base coordination rather than Si-O-Si condensation.
Raw Material Specifications Procurement Teams Must Enforce
When sourcing MPS or related dental-grade silanes from a chemical supplier, the following parameters are not negotiable for a product that will end up in a clinical primer:
| Parameter | Minimum Acceptable Specification | Why It Matters |
|---|---|---|
| Purity (GC) | ≥97% | Low-purity grades contain hydrolysis byproducts that compete for surface sites |
| Moisture content | <200 ppm | Premature hydrolysis and self-condensation during storage |
| Methoxy content | Per stoichiometric spec ±0.5% | Controls hydrolysis rate and silanol yield |
| Pre-condensed oligomers | Absent (confirm by GPC or viscosity) | Oligomers reduce active monomer concentration without signaling it |
| Hydrolysis rate | Tested and documented by supplier | Fast hydrolysis matters for single-application primers; slow rates suit two-bottle systems |
Suppliers who cannot provide a Certificate of Analysis with GC purity, moisture data, and oligomer absence confirmation should not be on the approved vendor list for dental formulations. The chemistry is unforgiving: a silane raw material that looks acceptable on basic specifications but carries 3–5% pre-condensed species will underperform in bond strength testing and may not reveal the cause until considerable R&D time has been spent chasing a formulation problem that is actually a supply chain problem.
Step-by-Step Surface Preparation Before Silane Application: Etching, Sandblasting, and Cleaning Protocols
Surface preparation is where most silane bond failures actually originate. The silane chemistry gets blamed, but the root cause is almost always what happened — or didn’t happen — to the ceramic surface in the 10 minutes before silane was applied. A clean, topographically activated surface with exposed silanol groups is what allows MPS or any other dental silane to form genuine covalent bonds. Skip or rush this phase, and even a well-formulated 3 wt% MPS primer is largely wasting its time.
Hydrofluoric Acid Etching: Ceramic Type Dictates Concentration and Time
For silica-based ceramics — feldspathic porcelain, leucite-reinforced glass-ceramic, and lithium disilicate — HF etching is the gold standard pre-treatment. The acid selectively dissolves the glassy silica matrix, exposing crystalline phases and creating a micro-retentive honeycomb topography. Crucially, this process also generates fresh silanol groups (Si–OH) on the surface, which are the actual reactive sites that allow silane to condense and bond.
The right concentration and duration depend on ceramic composition and firing density:
| Ceramic Type | HF Concentration | Etching Time | Notes |
|---|---|---|---|
| Feldspathic porcelain | 5–9% | 20–60 seconds | Longer times risk over-etching; check for matte finish |
| Leucite-reinforced (e.g., IPS Empress type) | 5–9% | 60 seconds | More resistant than feldspathic; verify frosted appearance |
| Lithium disilicate (e.g., e.max type) | 9–9.5% | 60–90 seconds | High acid resistance; under-etching is common mistake |
| Zirconia | Contraindicated | — | No silica phase; HF produces no benefit |
| Alumina-reinforced ceramic | Contraindicated | — | See airborne abrasion protocol below |
Over-etching feldspathic porcelain beyond 90 seconds at 9% HF can actually collapse the micro-retentive structure, reducing mechanical interlocking without adding more silanol groups. Etching time is not a parameter to improvise.

Why HF Is the Wrong Tool for Zirconia and Alumina Ceramics
Zirconia and alumina-reinforced systems contain no appreciable glassy silica phase. Applying HF does nothing useful to the crystalline ZrO₂ or Al₂O₃ lattice — it generates no topography, exposes no silanol groups, and in some cases introduces surface micro-damage that slightly reduces flexural strength. Bond failures on zirconia treated with HF are frequently misattributed to silane performance.
The correct approach is airborne-particle abrasion: 50 µm Al₂O₃ particles at approximately 2–2.5 bar pressure, applied in 10-second bursts at a standoff distance of roughly 10 mm. This creates mechanical retention through surface roughening and activates the surface by introducing compressive stress and surface energy changes. After abrasion, specialized silanes with phosphate or zirconate functional groups — not standard MPS — are required for meaningful chemical bonding. That chemistry is addressed in the previous section.
Post-Etch Cleaning: Removing Residue Without Recontaminating the Surface
After HF etching, the surface carries residual fluorosilicate reaction products and loose silica debris. Both block silanol sites. Ultrasonic cleaning in 95% ethanol or isopropanol for 3–5 minutes removes this contamination reliably. Water-only rinsing is insufficient — it clears fluoride residue but leaves organic contamination poorly addressed.
Saliva or blood contact after etching but before silane application significantly reduces bond strengthTrue
Organic contaminants adsorb onto freshly exposed silanol groups, occupying the same sites needed for silane condensation. Studies show shear bond strength can drop 40–70% when etched ceramic is contaminated prior to silanization, even with subsequent cleaning attempts.
Handle etched surfaces only with clean metal instruments. Glove powder, skin oils, and aerosol contamination in a busy clinical environment are real hazards. If contamination occurs after etching, re-clean ultrasonically — re-etching may be necessary if contamination was heavy.
Drying Protocol and the Contact Angle Standard
Oil-free compressed air at room temperature (18–25°C) is the correct drying method. The nuance here matters: a completely bone-dry surface is not ideal. A slightly humid surface — not visibly wet, but not desiccated — preserves the hydration layer that facilitates initial silanol condensation kinetics when the silane is applied. Over-drying with heated air or prolonged air blasting can reduce surface silanol reactivity.
A practical quality check is water contact angle measurement on the etched ceramic surface. A properly prepared surface should show a contact angle below 10° — close to complete wetting. Angles above 20–25° indicate contamination or incomplete etching and should trigger re-treatment before silane application proceeds.
Visual Inspection: The Matte Finish Test
Properly HF-etched feldspathic porcelain looks visibly different from an unetched surface. Under good lighting, a correctly etched area appears matte and frosted, not reflective. Glossy patches indicate incomplete acid penetration — typically caused by uneven HF application, insufficient contact time, or residual glazing from the original ceramic firing.
These glossy zones will show near-zero silane bond efficacy because the micro-retentive topography is absent and fresh silanol groups have not been exposed. Spot re-etching those areas, followed by full re-cleaning, is the correct response. Proceeding to silane application on a partially glossy surface produces a restoration with locally unpredictable bond strength — a scenario that leads to debonding failures that are preventable at this step.
How to Apply [Silane Coupling Agent](https://siliconchemicals.com/silane-coupling-agents/) to Dental Ceramics: Concentration, Timing, Drying, and Heat Activation
Getting the chemistry right in the lab means nothing if the application protocol is sloppy. Bond failures traced back to “bad silane” are, in the majority of cases, actually failures of concentration control, dwell time, or moisture recontamination. What follows is a protocol built from the actual physical chemistry of MPS hydrolysis and condensation — not a paraphrase of a product insert.
Preparing the Silane Solution from Bulk MPS
Most clinical silane primers arrive pre-formulated. If you are working with bulk 3-methacryloxypropyltrimethoxysilane (MPS, CAS 2530-85-0) — as a lab formulator or procurement-driven operation sourcing from a silane manufacturer — the working solution requires deliberate preparation.
A practical starting formulation: dissolve 2 g MPS into 95 mL of 95% ethanol combined with 5 mL distilled water. Add glacial acetic acid dropwise while stirring until the solution reaches pH 4.0–4.5, confirmed with a calibrated pH meter or at minimum a narrow-range pH strip. Then allow the solution to stand at room temperature for at least 30 minutes before any application. That hydrolysis window converts the methoxy groups (-OCH₃) to reactive silanols (-SiOH), which are the species that actually bond to the ceramic surface.
pH control here is not a suggestion. At pH above 5, hydrolysis rate drops sharply and you apply largely unreacted silane — covalent bonding to the ceramic will be minimal. At pH below 3.5, silanol groups condense rapidly with each other rather than with the ceramic, producing soluble oligomers and eventually silica particles. The effective bonding window is narrow. A solution sitting at pH 4.0–4.5 with a 30-minute hydrolysis period gives you a stable, reactive silanol population.
Application Technique
Use a clean, lint-free microbrush or a fresh foam applicator tip — never a cotton pellet, which sheds fibers and introduces contamination. Apply a generous, uniform coat across the entire etched ceramic surface in a single deliberate stroke. The goal is complete, even coverage. Do not allow the solution to pool at margins or in concavities; thick silane layers cure into a brittle, poorly cross-linked film that actually reduces shear bond strength compared to a thin, well-organized monolayer.
Apply two consecutive coats. Between coats, blow a brief stream of clean air across the surface for approximately 30 seconds — this removes excess solvent and any pooled solution without prematurely evaporating the reactive silanol layer you need for bonding.
Dwell Time: The Condensation Window
After the second coat, allow the silane to sit undisturbed on the ceramic surface for 60–180 seconds. This is the period during which Si-OH groups condense with surface silanol groups on the ceramic (-Si-OH ceramic) to form covalent Si-O-Si bonds. Rushing this step — blowing air immediately after application, as is common when clinicians are managing chair time — systematically reduces bond quality. The bonds that do not form in this window will not form later.
Skipping or shortening the silane dwell time below 60 seconds reduces ceramic-to-resin bond strengthTrue
Covalent Si-O-ceramic bond formation requires time for silanol condensation. Studies measuring shear bond strength at varying dwell times consistently show lower values when dwell is cut short, because the reaction is kinetically limited at room temperature.
Solvent Evaporation and Heat Activation
After the dwell period, evaporate residual solvent. A warm air stream from a dental air gun at approximately 50–60°C for 10–15 seconds is sufficient at chairside. For lab settings, placing the restoration in a drying oven at 100°C for 60 seconds is preferable — heat drives off adsorbed water, promotes further condensation of the silane layer, and increases cross-linking density within the film. The practical outcome: heat-activated silane treatments consistently show 15–30% higher shear bond strength compared to ambient air-dry alone, depending on ceramic type, silane concentration, and baseline surface roughness.
Do not substitute a heat gun aimed close to the surface — localized overheating above 150°C can degrade the methacrylate functional group, destroying the organic side of the coupling chemistry.
Visual Quality Check
A correctly treated surface looks uniformly matte and slightly dull. There should be no visible streaking, no glossy pooled areas, and absolutely no white powdery residue. White powder is a diagnostic sign: it indicates either over-concentration of the silane solution or premature bulk condensation, meaning you have deposited silica-like particles rather than a reactive film. If you see this, clean the surface back to bare ceramic — repeat the HF etch if needed — and re-treat with a fresh, correctly pH-adjusted solution.
Timing to Resin Cementation
Apply resin cement within 5–10 minutes of completing the silane application step. Silane-treated ceramic surfaces are vulnerable to moisture recontamination: ambient humidity and airborne contamination begin to hydrolyze the newly formed Si-O-Si bonds, and beyond 30 minutes at chairside conditions, measurable bond strength degradation occurs. If there is any delay — a patient management interruption, equipment issue — repeat the silane application from scratch rather than proceeding on a compromised surface. The extra two minutes is far cheaper than a de-bonded restoration at six months.
Silane Use in Specific Dental Procedures: Veneers, Crowns, Inlays, Composite Repairs, and Fiber Posts
The general protocol — etch, silanize, bond — holds across dental applications, but the details shift meaningfully depending on substrate chemistry, ceramic thickness, and whether you are working in a controlled lab or inside a patient’s mouth. Each scenario below carries its own failure mode if steps are compressed.
Feldspathic and Pressed Ceramic Veneers
Veneers represent the highest-stakes silane application in dentistry. At 0.3–0.7 mm thickness, the ceramic contributes almost nothing to fracture resistance on its own; the adhesive bond to enamel carries the mechanical load. The protocol is non-negotiable: 9.5% HF gel for 60–90 seconds on feldspathic porcelain, rinse thoroughly, dry, apply MPS silane (0.5–2 wt% in acidified ethanol, pH 4–5), allow 60 seconds dwell, air-dry, and heat-activate at 100–110 °C for 60 seconds where a lab oven is available. Target shear bond strength to resin cement should reach ≥20 MPa; untreated feldspathic porcelain bonded directly to resin typically tests at 4–8 MPa, which is clinically unreliable under lateral occlusal forces. Skipping heat activation can leave methanol and residual solvent trapped in the silane layer, reducing bond strength by 15–30% depending on ambient humidity during application.
Lithium Disilicate Crowns and Onlays
Lithium disilicate (LS2) ceramics contain roughly 57% SiO2 by weight, which means MPS silane bonds well to the silica phase after proper etching. The crystal-reinforced microstructure is denser than feldspathic porcelain, so HF exposure typically runs 20–60 seconds rather than the longer times some clinicians carry over from feldspathic habits — over-etching LS2 can damage surface integrity without improving bond area. Etched and silanized lithium disilicate routinely achieves 25–35 MPa shear bond strength to resin cement; the exact figure depends on cement type, silane concentration, and whether heat activation was used. This range is clinically sufficient for full-coverage restorations under normal occlusal loading.
Zirconia Crowns and Bridges
Zirconia contains no silica phase, so HF etching produces no surface topography worth bonding to. The effective protocol starts with airborne-particle abrasion (50 µm alumina, 2–4 bar) to create mechanical interlocking, followed by an MDP-containing zirconia primer. MDP bonds chemically to zirconia’s ZrO2 surface through phosphate-metal coordination. Some clinicians then apply an MPS silane layer over the dried MDP primer to provide a methacrylate coupling surface for the resin cement. Current in vitro evidence suggests this MDP + MPS combination offers modest additional bond strength compared to MDP primer alone — roughly 5–15% improvement depending on the resin cement used — but the benefit is not consistently reproduced across studies. For procurement and formulation teams: do not substitute a standard MPS silane-only primer on zirconia expecting feldspathic-level results; the chemistry simply does not match.
Standard HF etching improves bond strength to zirconia the same way it does for feldspathic ceramicsFalse
Zirconia (ZrO2) contains no silica phase. HF dissolves silicate glasses and creates microroughness on silica-containing ceramics; it has no comparable effect on zirconia surfaces and should not be used as a primary bonding step for zirconia restorations.
Intraoral Ceramic Repair
Repairing a chipped veneer or crown without removal requires adapting the protocol to a constrained, wet clinical environment. Clean the fracture surface with phosphoric acid (37%, 15–30 seconds) to remove contamination. If the site is accessible and isolation is reliable, apply HF gel cautiously — intraoral HF use carries soft-tissue burn risk and demands rubber dam isolation, petroleum jelly on surrounding gingiva, and strict time limits (30–60 seconds maximum). After thorough rinsing, apply MPS silane, allow dwell time, air-dry gently, apply bonding agent, and layer composite. Where HF is not safely accessible intraorally, airborne-particle abrasion through a micro-etcher is an acceptable alternative, accepting a modest bond strength reduction.
Glass Fiber Posts
Glass fiber posts have a silica-rich fiber matrix that responds well to MPS silane, giving them an advantage over metal or zirconia posts in adhesive cementation scenarios. Apply silane to the post surface for 60 seconds before insertion, allow solvent evaporation, then cement with dual-cure resin cement. In vitro studies consistently show silane treatment of fiber posts reduces post debonding rates by 30–50% compared to unsilanized controls; the actual improvement depends on post brand, fiber volume fraction, and the resin cement’s filler composition.
Chairside vs. Laboratory Application
Lab application is preferable when available: controlled temperature, heat oven access, and no time pressure from a patient in the chair. Chairside application — necessary for repairs and post cementation — requires compensating for the missing heat activation step by extending silane dwell time to 90–120 seconds and ensuring thorough solvent evaporation with clean, dry air before bonding agent placement. Humidity above 60% RH measurably slows silane condensation reactions; in humid operatories, a brief warm air stream (not hot) helps drive off adsorbed water from the ceramic surface before silane contact.
Hydrolytic Stability and Aging: How Silane Bonds Degrade in the Oral Environment and How to Maximize Long-Term Durability
The oral cavity is one of the most chemically aggressive environments any adhesive bond will ever face. Temperature swings from hot coffee to ice water, pH excursions from a soda at 3.0 to a post-meal alkaline saliva spike near 8.5, salivary enzymes including esterases and amylases, and the relentless mechanical fatigue of occlusal loading — all of these act simultaneously on the Si-O-ceramic interface. Clinicians and lab technicians who attribute late-stage restoration failures to cement or porcelain quality are frequently looking in the wrong place. The silane bond itself is degrading.
The Thermocycling Evidence and What It Actually Means
Standardized thermocycling protocols — 5°C to 55°C, simulating years of clinical function — consistently show shear bond strength reductions of 20–50% after 10,000 cycles relative to 24-hour baseline values. The exact magnitude depends on ceramic type, silane concentration, whether heat activation was used, and whether a hydrophobic sealer was applied. Feldspathic porcelain loses bond strength faster than lithium disilicate under the same protocol, largely because its silica surface chemistry is more uniform and therefore more uniformly attacked. The practical implication is straightforward: a restoration that passes an initial laboratory pull test is not guaranteed to maintain that performance across five to ten years of service.
Where the Bond Actually Breaks Down
Water molecules attack Si-O-Si linkages in a reversible hydrolysis reaction. The weakest point in the assembly is almost never inside the resin matrix — it is at the silane monolayer-to-ceramic-oxide interface, where surface hydroxyl groups compete with the siloxane bond for water. Excess silane application makes this worse. Multilayer silane deposits, formed when concentration is too high or evaporation is incomplete, create a condensed silicone film with internal Si-O-Si bonds that hydrolize preferentially, causing the entire overlying structure to delaminate as a unit. An optimized, well-formed monolayer — achieved by the concentration and drying protocols covered earlier in this article — is genuinely more durable than a thick application that looks more thorough.

Four Strategies That Demonstrably Extend Bond Life
Heat activation at 100–150°C for 60–90 seconds drives condensation of residual silanol groups into covalent Si-O-Si bonds with the ceramic substrate, meaningfully increasing the proportion of bonds that resist hydrolytic attack. This single step consistently separates aged bond performance between heat-activated and air-dried samples in comparative studies.
Silane chemistry selection matters at the procurement and formulation level. Bis-silane structures and MPS variants with slightly bulkier organosilicon backbone geometries show improved hydrolytic stability compared to standard single-alkoxysilane configurations. If your restoration involves zirconia, coupling silane with an MDP phosphate primer creates a Zr-O-phosphate anchor as the primary bond — that MDP-Zr-O bond is substantially more resistant to hydrolysis than the Si-O-Zr bond that silane alone would attempt to form.
Applying a thin, hydrophobic resin sealer over the silanized surface before cementation acts as a moisture exclusion barrier during the critical early loading period. This is a low-cost step that procurement teams rarely specify but lab protocols should.
Storage, Contamination, and the Re-Silanization Protocol
Re-applying silane over an aged or contaminated silane layer restores bond strength adequately.False
Aged silane layers contain hydrolyzed, condensed silicone residues that physically block new silane from reaching the ceramic oxide surface. Full re-etching — HF acid for silica-based ceramics, alumina sandblasting for zirconia — is required to expose fresh hydroxyl groups before re-silanization. Skipping this step produces an adhesive interface with unpredictable and typically reduced bond strength.
A silanized restoration sitting on the bench is not stable. Exposure to ambient humidity at 60–70% relative humidity for more than 24 hours measurably degrades silane effectiveness. Store silanized restorations in a sealed, dry container, away from light. If cementation is delayed beyond a working day, treat the piece as unsilanized: clean, re-etch, and re-apply silane from scratch.
Contact Angle as a Practical Quality Check
A freshly silanized ceramic surface with methacrylate groups properly oriented toward the resin should show a water contact angle of 50–70°. Clean etched ceramic before silanization typically reads below 10° — almost perfectly wettable. The hydrophobic shift is the indicator that silane coverage is adequate and oriented correctly. This is a bench-level test any lab can perform with a syringe and a photograph; it takes under two minutes and eliminates guesswork about whether a batch of silane primer is still performing or has degraded in storage.
Formulating Dental Silane Primers: Raw Material Specifications and Quality Control for Manufacturers
Dental primer performance starts at the raw material specification sheet, not at the mixing bench. If you are purchasing bulk 3-methacryloxypropyltrimethoxysilane (MPS, CAS 2530-85-0) to produce a commercial dental silane primer, the quality parameters you set on incoming material will determine every downstream formulation and shelf-life outcome. Accepting a borderline lot to save margin on a small batch is the single fastest way to generate a bond-strength failure complaint six months post-launch.
Raw Material Specification for Dental-Grade MPS
The minimum acceptable purity for dental applications is ≥98% by gas chromatography. Refractive index at 20°C should fall between 1.428 and 1.432; anything outside that window signals either incomplete synthesis or contamination with hydrolysis products. Density at 20°C should read 1.044–1.047 g/mL — this is a quick incoming inspection check that takes under two minutes and will catch diluted or mislabeled drums before they enter production.
Moisture content is the specification most frequently underweighted by procurement teams. Karl Fischer titration must confirm 15 MΩ·cm — standard RO water is not acceptable). pH is adjusted to 4.0–4.5 with glacial acetic acid, which catalyzes hydrolysis of the methoxy groups to silanols without driving condensation into oligomers at the concentrations used.
| Component | Typical Range | Critical Dependency |
|---|---|---|
| MPS (≥98% GC purity) | 1.0–2.0 wt% | Higher end for zirconia substrates |
| Ethanol (95%, pharma grade) | 90–95 wt% | Must be low-water feedstock |
| Deionized water (>15 MΩ·cm) | 3–5 wt% | Controls hydrolysis rate |
| Glacial acetic acid | 0.05–0.20 wt% | Adjust to pH 4.0–4.5 |
| MEHQ stabilizer | 80–120 ppm | Scale with MPS load |
Two-Bottle vs. Single-Bottle Product Architecture
The two-bottle system stores MPS in anhydrous ethanol (Bottle A) and acidified aqueous solution (Bottle B) separately. Mixed immediately before use, this format reliably achieves 18–24 month shelf life at 15–25°C because hydrolysis and condensation cannot proceed while the silane and water are physically separated. Once mixed, pot life is typically 30–60 minutes, which must be printed on the label.
Pre-hydrolyzed single-bottle formats are commercially convenient but chemically fragile. The instability mechanism is straightforward: hydrolyzed silanols undergo intermolecular condensation over time, building siloxane oligomers that no longer have free silanol groups to bond to the ceramic surface. Bond strength falls progressively after formulation, often well before the printed expiry date. To extend single-bottle stability to 12 months, formulators use co-solvents such as isopropanol or methanol to slow condensation kinetics, and buffer the pH tightly at 4.0–4.2 rather than relying on a single acetic acid addition. Some manufacturers incorporate dilute organotitanate catalysts at ≤50 ppm to improve silanol reactivity at the point of use while keeping storage-phase condensation suppressed. Cold-chain storage at 2–8°C is then mandatory, not optional.
Pre-hydrolyzed single-bottle dental silane primers maintain equivalent bond strength to two-bottle systems throughout their labeled shelf life when stored at room temperature.False
Single-bottle pre-hydrolyzed formulations undergo progressive silanol condensation at ambient temperature, reducing available reactive silanols over time. Without cold-chain storage and tightly controlled pH buffering, shear bond strength can drop measurably within 3–6 months, well before a 12-month expiry date. Two-bottle systems avoid this entirely by keeping water and MPS separated until use.
Critical QC Tests for Finished Dental Silane Primer
Release testing should include pH measurement (4.0–5.0 pass range), GC quantification of residual MPS against a calibration standard, and Karl Fischer water content. These three tests take under four hours and catch the most common formulation deviations.
Functional performance testing requires shear bond strength testing on etched feldspathic porcelain bonded to a standard composite resin under ISO 29022 or equivalent protocol — the acceptance criterion is ≥18 MPa. Contact angle measurement on etched ceramic after primer application should fall at 50–70°; a contact angle below 40° usually indicates over-hydrolysis or excessive water content, while above 75° suggests incomplete silanol formation or surface contamination.
Accelerated aging at 40°C and 75% relative humidity for 3 months is the minimum stability study for regulatory submission. Samples at 0, 4, 8, and 12 weeks are re-tested for pH, MPS content by GC, and shear bond strength. Any single parameter falling outside specification range at the 8-week point is a formulation red flag, not an isolated data point.
Regulatory and Biocompatibility Documentation
Dental silane primers enter the market as dental materials and are subject to ISO 10993 biocompatibility testing. MPS itself carries an oral LD50 >5,000 mg/kg in rats and is REACH registered, but the finished formulation — including all excipients, solvents, and stabilizers — must be tested for cytotoxicity per ISO 10993-5 and confirmed non-mutagenic by Ames test or equivalent. CE marking under EU MDR requires a complete technical file including biocompatibility data, clinical evidence, and post-market surveillance plan. FDA 510(k) clearance for dental primers typically relies on substantial equivalence to a predicate device, and the biocompatibility data package mirrors the ISO 10993 battery in scope.
Packaging and Storage
Finished primer must be packaged in amber glass or natural HDPE bottles to block UV-initiated methacrylate polymerization. The headspace should be nitrogen-blanketed at fill — this is not a precaution that can be skipped for cost reasons, because oxygen depletion during storage accelerates MEHQ consumption and leaves the methacrylate group unprotected. Two-bottle products store well at 15–25°C; single-bottle pre-hydrolyzed formats require 2–8°C cold chain throughout distribution. Labels must state mix ratio, pot life after mixing, storage temperature, and expiry date. An unlabeled pot life is a regulatory deficiency and a clinical hazard.
Troubleshooting Silane Bonding Failures: Diagnosing and Correcting the 8 Most Common Errors
Silane chemistry works reliably when conditions are controlled. When it fails, the failure mode is rarely random — each root cause leaves a recognizable fingerprint. The eight errors below account for the vast majority of clinical debondings and lab-scale bond strength failures seen in practice.

Error 1 — Insufficient HF Etching Time or Concentration
Under-etching leaves the ceramic surface optically smooth and chemically inert. The silane has nowhere to anchor. Diagnosis is straightforward: a properly etched feldspathic or leucite-reinforced surface looks uniformly frosted under oblique light; a glassy or patchy surface after “etching” means the HF either ran out of active concentration or the dwell time was cut short. Fresh 5–9% HF gel on feldspathic porcelain needs 60–90 seconds; lithium disilicate typically requires only 20 seconds at 5% — longer contact with stronger acid destroys the microstructure rather than developing it. Discard partially used HF containers that have been open more than a few weeks; buffering from atmospheric CO₂ and absorbed water progressively drops effective fluoride activity.
Error 2 — Silane Applied to a Contaminated Surface
Saliva protein, blood, die spacer, or residual polishing paste physically blocks the silanol sites you created by etching. The silane solution beads up rather than spreading — contact angle above roughly 30° on a freshly etched surface is an immediate warning sign that contamination is present. Ultrasonic cleaning in fresh 99% ethanol for 3–5 minutes followed by air-drying, then re-etching and re-silanizing, is the only reliable correction. Wiping with a cotton roll is not sufficient; polishing paste residue in particular embeds into the microporosity the HF just opened.
Error 3 — Expired or Improperly Stored Silane
MPS silane in aqueous ethanol is a living system. Stored above 25°C, exposed to light, or past its shelf date, it undergoes self-condensation into polysiloxane oligomers that are already crosslinked and cannot form new covalent bonds with the ceramic surface. A turbid solution, visible viscosity increase, or any gel-like texture means the product is inactive — not marginal, but essentially inert. Discard it. There is no way to reverse siloxane oligomer formation in the bottle. Implement strict FIFO rotation and store silane primers below 15°C, away from light. Shelf life for opened containers runs 3–6 months depending on formulation; unopened, properly cold-stored MPS solutions typically hold 12–24 months, but verify the specific supplier’s certificate of analysis.
Pre-condensed (polymerized) MPS silane cannot form effective covalent bonds with ceramic surfaces and will not recover bond strength with extended application time.True
Once MPS undergoes self-condensation to form polysiloxane oligomers in solution, the reactive trimethoxysilyl groups are consumed. No covalent Si-O-ceramic linkage can form. The only correction is replacing the product.
Error 4 — Wrong Silane Product for Zirconia
Zirconia contains no free silica. MPS-only primers depend entirely on Si-OH condensation chemistry — they have no reactive pathway on a zirconia surface. The failure pattern is adhesive fracture cleanly at the ceramic-cement interface with no cohesive component, typically presenting within 6–18 months clinically. The correction is not more silane; it is switching to an MDP-containing zirconia primer protocol. MDP (10-methacryloyloxydecyl dihydrogen phosphate) bonds to zirconia through phosphate-Zr coordination. Some formulations combine MDP with a silane for alumina-containing or hybrid ceramics, but for monolithic zirconia, MDP activity is what matters.
Error 5 — Silane Layer Too Thick
Pooled silane dries into a multilayer polysiloxane film. The outer layers are not bonded to the ceramic — they are only bonded to each other through weak van der Waals forces. When stress is applied, fracture runs through this weak cohesive layer, not at the cement or ceramic interface, which misleads the technician into suspecting the wrong variable. White residue, uneven sheen, or visible puddles after drying are diagnostic. Wipe off the excess immediately with a dry lint-free tissue, then apply a single thin, uniform coat from a fresh applicator. If the surface has dried with visible residue already, clean back to ceramic with ethanol, verify the etch is still intact, and repeat from silanization.
Error 6 — Skipping or Inadequate Heat Activation
Solvent evaporation and Si-O-ceramic bond completion both require thermal energy. Air-drying at room temperature leaves residual ethanol and water trapped in the silane film, and condensation reaction rates at 20°C are slow enough that cementation catches the interface in an incompletely bonded state. A standardized heat gun or bench oven at 100°C for 60 seconds is the minimum reproducible protocol. Do not substitute ambient air for more than 5 minutes — it does not achieve equivalent conversion regardless of extended time. In lab settings where QC bond strength testing shows high scatter, skipped or inconsistent heat activation is frequently the uncontrolled variable.
Error 7 — Excessive Delay Between Silanization and Cementation
A silane-treated surface begins rehydrating from ambient air within minutes. Bond strength loss of 30–50% between a 5-minute and 24-hour delay before cementation has been reported across multiple substrate studies. Clinically, this translates to a restoration that tests fine on the bench but debonds at 12–24 months. The working rule is: cement within 10 minutes of silane application. If the clinical workflow forces a longer delay — patient anesthesia issues, assistant handoff, impression retake — do not assume the silanized surface is still adequate. Repeat the silane step with fresh solution before cementation.
Error 8 — pH Outside the Optimal Hydrolysis Window
MPS silane hydrolyzes and forms active Si-OH groups between approximately pH 4 and 5. Below pH 3, self-condensation rate accelerates sharply and the solution degrades rapidly even in the bottle. Above pH 6, hydrolysis is too slow to generate adequate reactive groups before application. Both failure modes produce reduced bond strength, but they look different: very acidic solutions often appear clear while being partially self-condensed; near-neutral solutions may look normal while delivering incomplete hydrolysis. Check every production batch with a calibrated precision pH meter — a strip test does not give sufficient resolution at this range. If pH is out of specification, reformulate; do not attempt to correct by adding acid or base to an existing batch, because that changes the silane-to-solvent balance unpredictably.
| Error | Fast Field Diagnosis | Minimum Corrective Action |
|---|---|---|
| Insufficient HF etch | Glossy surface post-etch | Re-etch, fresh HF, correct time per ceramic type |
| Surface contamination | Silane beading, high contact angle | Ultrasonic ethanol clean, re-etch, re-silanize |
| Expired silane | Turbid or viscous solution | Discard; FIFO stock rotation |
| Wrong product for zirconia | Clean adhesive failure at cement interface | Switch to MDP-containing zirconia primer |
| Silane layer too thick | White residue, uneven sheen | Wipe excess, apply thin coat; or restart |
| No heat activation | High scatter in bond strength QC | Standardize 100°C / 60 s as mandatory step |
| Delayed cementation | Temporal debonding pattern | Cement within 10 min; repeat silane if delayed |
| pH out of range | QC bond failure, no obvious visual sign | Verify pH 4–5 with precision meter; reformulate |
Frequently Asked Questions About [Silane Coupling Agents](https://siliconchemicals.com/silane-coupling-agents/) in Dentistry
Can I use industrial-grade MPS instead of dental-grade silane primer?
Not recommended — at least not without formulation work and regulatory validation. Industrial MPS (CAS 2530-85-0) typically targets ≥97% purity, but the residual fraction matters: heavy-metal traces, unreacted methoxy groups, and byproduct siloxanes that are acceptable in a glass-fiber sizing operation are not acceptable in a material that contacts oral tissue. Dental-grade silane primers require controlled hydrolysis pH (4–5, acetic acid buffered), biocompatibility testing under ISO 10993, and documented batch-to-batch consistency.
That said, high-purity MPS at ≥98% from a qualified supplier — with full CoA, low heavy-metal limits, and traceable synthesis — is a legitimate starting point for a manufacturer formulating their own dental primer. The silane itself is not the barrier; the formulation, QC, and regulatory pathway are. Procurement teams sourcing bulk MPS for dental applications should specifically request dental-application data sheets and ask about impurity profiles, not just headline purity.
How long does a silanized ceramic surface stay bondable?
Cement it within 5–10 minutes. Bond strength begins declining measurably after that window: expect a 15–25% reduction at 30 minutes of ambient exposure, and losses approaching 50% after 24 hours as the reactive methacrylate groups oxidize, attract airborne contaminants, and the silane layer partially rehydrates. If any delay beyond 10 minutes is unavoidable, reapply silane and re-dry — do not attempt to cement a surface that has been sitting out.
Bond strength of silane-treated ceramics drops by 15–50% after 30 minutes to 24 hours of ambient exposure.True
This range is consistently reported across in vitro bond strength studies measuring shear bond strength at various time points post-silanization; the actual loss depends on humidity, temperature, and whether the surface was covered.
Does silane work equally on all dental ceramics?
No — and confusing substrate type is one of the costliest clinical errors in restorative dentistry. Silica-rich ceramics (feldspathic porcelain, leucite glass-ceramic, lithium disilicate) respond very well to HF etching followed by MPS silane because the etch creates micro-retentive topography and exposes silanol groups that form genuine Si-O-Si covalent bonds with the silane. Alumina and zirconia ceramics lack those reactive silica sites. MPS silane applied to zirconia produces little more than weak physisorption — clinical bond strengths are unreliable. These substrates need MDP-based primers or zirconia-specific surface treatments.
Why does heating the silane layer improve bond strength?
Air-drying at room temperature leaves residual ethanol and water trapped in the silane film and leaves condensation reactions incomplete. Heating to 100–150°C for 1–2 minutes drives off those solvents, accelerates Si-O bond condensation to the ceramic surface, and increases cross-link density within the organosilane layer itself. The practical result: studies consistently show 15–30% higher initial shear bond strength and meaningfully better hydrolytic aging resistance compared to air-dried controls. In a humid clinical environment where restorations cycle through acidic foods, saliva, and temperature swings daily, that aging resistance matters far more than the initial number.
How should dental silane primers be stored?
Single-bottle pre-hydrolyzed products are the most shelf-sensitive: store in original sealed amber glass at 2–8°C, use within 12 months, and inspect for turbidity before every use — cloudiness indicates silane oligomerization and the bottle should be discarded. Two-bottle systems (separate silane and activator combined at chairside) are more stable at room temperature, 15–25°C, with shelf lives typically reaching 24 months. Never store any silane primer in direct sunlight or near solvents that could compromise the cap seal.
What distinguishes a silane primer from a ceramic primer or bond system?
A silane primer contains the coupling agent only — it creates the chemical bridge to silica-based ceramic surfaces and requires a separate resin cement on top. A ceramic primer or universal ceramic bond system combines silane with a phosphate monomer (most commonly MDP) and sometimes additional adhesive resins, targeting broader substrate compatibility including zirconia and alumina in a single product. For purely silica-based ceramics, standalone silane primer before resin cement is fully sufficient and often preferable because it keeps each layer’s chemistry clean and auditable. The combined systems earn their value when you are bonding across mixed or uncertain substrates.
How do I verify that silane application was successful before cementing?
The water contact angle test is the most reliable quick check. Apply a small droplet to the treated surface: an angle of 50–70° confirms proper silane coverage with methacrylate groups oriented outward toward the resin cement. An angle below 30° suggests incomplete drying or silane failure; above 80° suggests contamination. Visually, a correctly silanized feldspathic ceramic surface appears uniformly matte — no pooling, no shiny wet zones, no white powdery residue from silane over-application.
Can silane treatment repair a debonded ceramic veneer that is still intact?
Yes, but only if the failure mode is correctly identified first. Examine both the veneer’s intaglio surface and the tooth preparation: if the failure was at the ceramic-cement interface (clean ceramic surface with cement remaining on tooth), re-etching with HF, re-silanizing, and re-cementing is a rational repair. If the failure was cohesive within the cement layer or at the tooth-cement interface, re-silanization alone solves nothing — the adhesive protocol for dentin or enamel also needs revision. Skipping this diagnostic step and simply re-silanizing results in repeat failure at the same weak link.
Sourcing Dental-Grade Silane Coupling Agents: What Global Buyers Should Evaluate When Selecting a Supplier
Procurement decisions for dental-grade silane look deceptively simple on paper — it is a single monomer, widely available, with a well-known CAS number. In practice, the gap between a compliant-looking specification sheet and a silane that actually performs reliably in a dental primer formulation is wide enough to cost a manufacturer months of failed validation work. What follows is a working checklist built around what actually separates adequate from genuinely qualified supply.
Chemical Specifications That Matter — and Why Each One Does
Start with GC purity. For 3-methacryloxypropyltrimethoxysilane (MPS, CAS 2530-85-0), require ≥98% purity on a lot-specific certificate of analysis with actual measured values — not a printed specification range. Impurities, particularly hydrolysis by-products from poor storage or process control, consume bonding sites on the ceramic surface and dilute effective silane concentration in your primer. Bond strength losses of 15–30% have been documented in lab studies comparing 96% vs. 99% MPS lots under identical formulation conditions.
Karl Fischer moisture content should be confirmed at <200 ppm per lot. MPS hydrolyzes in the presence of water even before it reaches your formulation vessel. Pre-hydrolyzed silane forms oligomeric siloxane networks — silanol condensation products that no longer have functional trimethoxysilyl groups available for ceramic surface bonding. A moisture report stating “passes specification” without a numeric value is not acceptable; you need the actual measured figure.
Request 29Si NMR or GC-MS data specifically to confirm absence of pre-hydrolyzed dimers and trimers. This is the test many lower-tier suppliers cannot run. If a supplier cannot provide this data or declines to offer it, treat that as a disqualifying signal. The methacrylate inhibitor content (MEHQ, typically 50–200 ppm depending on grade) also requires its own certificate — too little and the monomer polymerizes prematurely in storage; too much and it interferes with free-radical cure in your primer system. Refractive index and density, reported lot-specifically, provide a rapid incoming QC fingerprint that catches gross substitution or contamination before any advanced testing.

Regulatory Documentation for Dental Manufacturer Submissions
MPS is registered under REACH (the EC inventory number commonly cited is 231-248-0 for the silicate precursor class; confirm current registration status with your supplier directly for the specific REACH registration number applicable to your import jurisdiction). Require a current GHS/UN-compliant SDS, ISO 9001 manufacturing certification with scope coverage for specialty silane synthesis, and — critically for dental material manufacturers preparing FDA 510(k) submissions or CE technical files — ask whether the supplier can provide raw material characterization data packages or support a Drug Master File reference. Few Chinese suppliers offer formal DMF filing, but a well-documented raw material characterization package (impurity profiles, stability data, manufacturing process summary) can satisfy most notified body and FDA reviewer requests for dental device raw material traceability.
MPS (CAS 2530-85-0) is registered under the REACH regulation, making it legally importable into the EU when sourced from a compliant supplier with valid registration documentation.True
REACH requires registration of chemical substances imported into or manufactured in the EU above 1 tonne/year. MPS is a listed substance; confirmed registration documentation from the supplier is a mandatory compliance requirement for EU dental material manufacturers.
Evaluating Supply Chain Reliability
Batch-to-batch consistency matters more than single-lot performance. Request six-lot trend data on purity and moisture before committing to a supplier relationship. The numbers to watch are not just the averages but the ranges — a supplier showing ±0.3% purity variation across six lots is meaningfully more consistent than one showing ±1.5%, even if both means are ≥98%.
Standard lead times from qualified Chinese manufacturers run 4–6 weeks for stock grades; expedited orders can typically compress to 2–3 weeks at a price premium of 10–25% depending on freight mode and lot size. MOQs for dental-grade MPS vary — expect 25–50 kg minimums from specialty producers and 200 kg minimums from large commodity silane plants. For a dental primer manufacturer running small production batches, the former is almost always the right source. Confirm cold chain capability if your supplier ships through summer or to regions with high ambient temperatures; MPS has a flash point around 96°C but thermal exposure during transit accelerates inhibitor depletion and moisture uptake.
China’s Integrated Organosilicon Industrial Clusters
China’s Shandong, Zhejiang, and Guangdong provinces host vertically integrated organosilicon clusters where upstream silicon metal smelting and methylchlorosilane synthesis feed directly into downstream specialty silane production. This vertical integration — versus the fragmented toll-manufacturing model common in Western specialty chemical supply — is what enables cost advantages of roughly 20–40% compared with European or North American equivalents for the same specification. That cost advantage is real and structural, not a sign of quality compromise, provided the supplier operates with full analytical QC capability. The distinction that matters is not geography; it is whether the manufacturer runs GC, Karl Fischer, NMR, and lot-specific COA generation as standard practice rather than on request.
Red Flags That Should End Supplier Conversations Quickly
Any supplier who provides a COA with only specification limits and no measured values is printing documentation, not measuring product. No 29Si NMR capability is a serious gap for a dental-grade supplier — this is not exotic equipment, and its absence suggests the analytical infrastructure required for high-specification applications is simply not there. Pricing significantly below prevailing market rates (more than 25–30% under current spot for MPS at ≥98%) almost always reflects a purity compromise, an inhibitor level outside the effective range, or moisture control failures. None of these are recoverable at the formulation stage without significant rework cost.
A Practical New-Supplier Qualification Protocol
Request a 500 mL sample before any volume commitment. Run GC purity and Karl Fischer moisture in-house first — these two tests take less than a day and screen out most unqualified lots immediately. Formulate into your standard dental primer at your working concentration (typically 1–3 wt% MPS in ethanol/water with acetic acid at pH 4–5). Measure contact angle on HF-etched feldspathic ceramic; target 50–70° confirms adequate surface coverage without excess. Run shear bond strength against BisGMA resin cement on feldspathic porcelain specimens. A qualified lot should consistently deliver ≥20 MPa. Repeat this across three separate sample lots from the same supplier. Only three consistent passing results — not one — should advance a supplier to approved status. The cost of this qualification protocol is small relative to the cost of a reformulation cycle or a field recall traced back to raw material variability.














