
A maintenance technician develops a persistent cough after weeks of working near a silicone oven-curing line. A formulator starts getting headaches during pilot batches of a new PDMS-based adhesive. A compliance officer fields a supplier notification about D5 content in a wash-off product — and doesn’t know whether it triggers a reformulation obligation or just a paperwork update. None of these situations announces itself loudly. Silicone toxicity rarely presents as an acute, unmistakable event; it surfaces as a slow pattern of respiratory irritation, regulatory exposure, or environmental liability that operations teams attribute to something else for months. By the time the pattern is traced back to a silicone material — a cyclosiloxane volatilizing from a heated bath, chlorosilane residues in a poorly ventilated mixing room, silica particulate from combustion above 450°C — the occupational illness claim is already open, the REACH notification obligation is already overdue, or the wastewater consent condition is already in breach. The financial consequence compounds: a single OSHA willful violation can reach $156,259 per citation, average occupational illness claims in US chemical manufacturing run $40,000–$150,000, and product reformulation triggered by a missed regulatory threshold carries costs that dwarf the original compliance spend.
Silicone toxicity signs range from acute respiratory and skin irritation — caused by reactive intermediates like hydrogen chloride from chlorosilane hydrolysis — to chronic, low-visibility effects from cyclosiloxane exposure (D4, D5), including endocrine disruption, bioaccumulation, and environmental persistence. Processing temperature, molecular weight, and regulatory jurisdiction determine which hazard applies and at what threshold.
What makes this subject genuinely difficult — and genuinely dangerous for industrial users — is that the word “silicone” covers a family of chemically distinct materials with very different risk profiles. Fully cured, high-molecular-weight PDMS in a food-contact or medical application sits at one end of the spectrum, carrying FDA 21 CFR 175.105 clearance and ISO 10993-13 biological evaluation frameworks. Cyclic volatile siloxanes, chlorosilane precursors, and thermally degraded silicone at the other end are subject to REACH SVHC designations, California Prop 65 reproductive toxicity listings, and NIOSH ceiling exposure guidance. The gap between those extremes is where most industrial incidents and compliance failures actually live — in the processing steps, the intermediate materials, and the operating conditions that push an otherwise benign polymer into a hazardous state.

Silicone Chemistry Fundamentals: Why Bulk Polymer Toxicity Differs Radically from Small-Molecule Siloxane Exposure
The single most consequential mistake in industrial silicone hazard assessment is treating “silicone” as a single chemical entity. It is not. What arrives at a manufacturing site under that label may be a high-molecular-weight polymer with negligible biological activity, a mixture containing regulated cyclic oligomers, a reactive silane coupling agent capable of generating corrosive gas on contact with humidity, or a catalyst-crosslinked system whose tin-based cure chemistry carries its own distinct toxicological profile. Conflating these is how plants end up with the wrong PPE program, wrong ventilation design, and wrong medical surveillance protocol — and it is how occupational illness cases go undiagnosed for months because nobody connected a hepatic enzyme elevation to the RTV sealant in the maintenance bay.
PDMS: Why High-Molecular-Weight Silicone Is Not the Primary Hazard
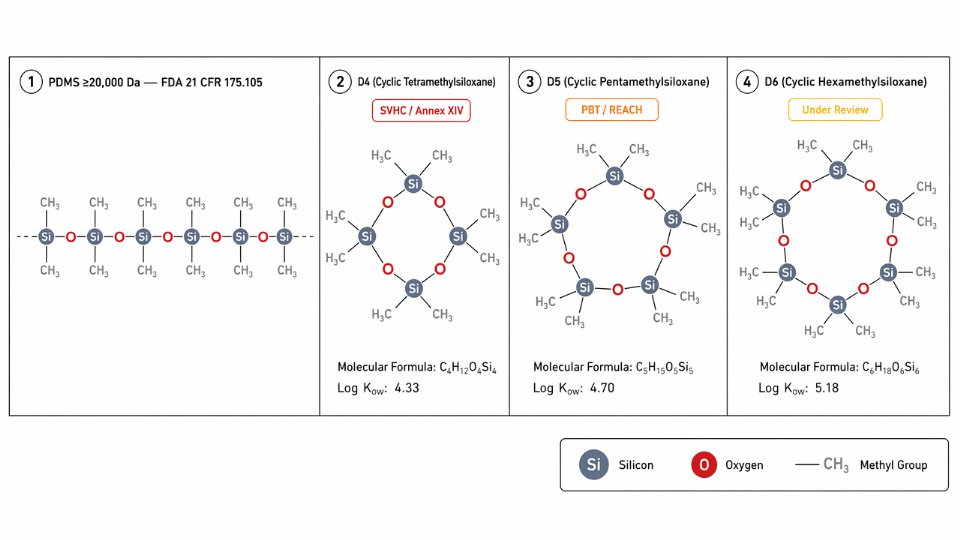
Polydimethylsiloxane (PDMS) — the Si–O backbone polymer that forms the bulk of silicone fluids, elastomers, and gels — is genuinely low in systemic toxicity at high molecular weight, and the mechanism is straightforward: poor membrane permeability, negligible oral and dermal absorption, and no documented receptor-binding activity at physiologically relevant concentrations. The Si–O–Si backbone is hydrophobic and chemically stable at body temperature, and the molecule is too large to cross biological membranes efficiently. FDA 21 CFR 175.105 clearance for food-contact applications is a useful regulatory proxy for this low systemic risk, though it is not a zero-toxicity declaration and applies specifically to high-MW grades, not to cyclic fractions or reactive intermediates. Engineers referencing the FDA clearance as a blanket safety certificate for all silicone chemistries are misreading its scope.
Cyclic Siloxanes: The Residual Fraction That Carries Regulatory Weight
The real toxicological concern in most industrial silicone exposures is not the polymer matrix — it is the low-molecular-weight cyclic oligomers, designated D3 through D6, that remain as process residuals in incompletely stripped or thermally degraded silicone. D4 (octamethylcyclotetrasiloxane) has been on the EU REACH Annex XIV authorization list since 2018 and is subject to restriction in wash-off cosmetic products above 0.1% w/w. D5 (decamethylcyclopentasiloxane), with a log Kow of 8.03, is classified as PBT (persistent, bioaccumulative, and toxic) under REACH and remains under active endocrine disruption scrutiny. D6 is under parallel review. These species volatilize readily at processing temperatures and are the fraction that occupational hygienists are actually measuring when they sample silicone oven or mixing environments.
In a typical elastomer compounding operation running three shifts, the steady-state ambient D4/D5 concentration near an open mixing bowl may remain below detection during routine throughput — then spike transiently during purging or cleaning cycles when residual volatiles are released in bulk. Operators often compensate by increasing general ventilation rather than addressing the point-source release, which dilutes the reading during shift monitoring but leaves peak exposures uncontrolled.
High-MW PDMS is biologically inert and carries no occupational health risk in any formFalse
High-MW PDMS polymer itself has negligible systemic toxicity, but commercial silicone products contain residual cyclic oligomers (D4, D5), reactive silane components, and catalyst systems that carry independent and well-documented regulatory classifications. The polymer fraction and the product mixture are not the same thing.
Reactive Silanes: Acute and Chemical-Burn in Character
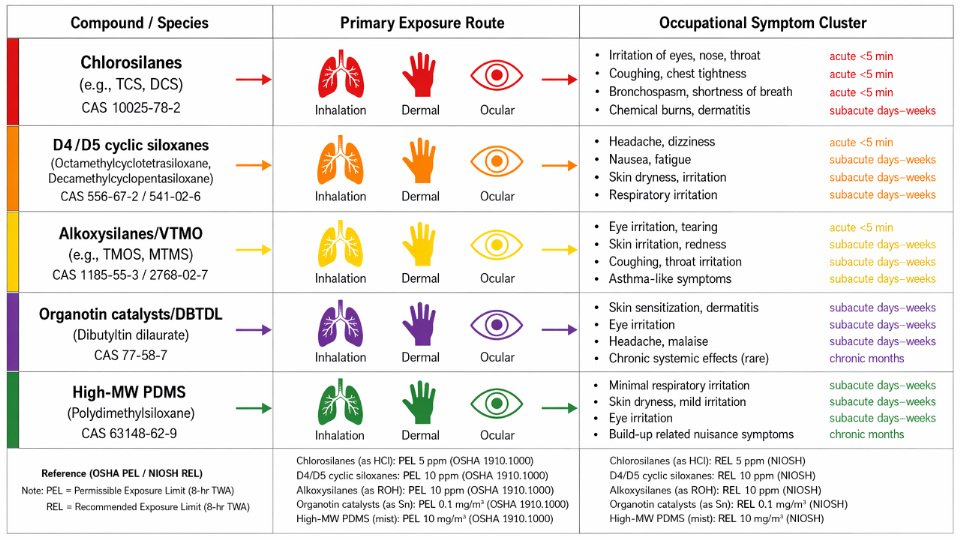
Functional silane coupling agents — vinyltrimethoxysilane (VTMO), aminopropyltriethoxysilane (APTES), and their analogs — occupy a distinct hazard class entirely. Alkoxysilanes hydrolyze on contact with atmospheric moisture, releasing methanol or ethanol as byproducts; the irritant effect is meaningful in confined spaces but generally manageable with standard ventilation. Chlorosilanes are significantly more acute: hydrolysis generates HCl gas, and signs of chlorosilane overexposure are chemical-burn in character — immediate upper respiratory irritation, lacrimation, and mucous membrane inflammation — not the slow, chronic, hard-to-trace pattern seen with cyclic siloxane accumulation. OSHA’s ceiling for HCl is 5 ppm, and a chlorosilane spill in an enclosed drum-handling area can breach that threshold within seconds of liquid contact with humidity.
Organotin Catalysts: The Hidden Driver Behind Attributed Systemic Signs
Condensation-cure and RTV silicone systems commonly use dibutyltin dilaurate (DBTDL) or dioctyltin dilaurate (DOTL) as crosslinking catalysts. These organotin compounds carry hepatotoxic and immunotoxic profiles independent of any silicone component — yet when a worker reports fatigue, elevated liver enzymes, or immune dysregulation after silicone handling, the organotin catalyst is frequently the last thing investigated. Organotin residues are detectable in cured silicone by ICP-OES at ppb concentrations; migration under heat or extraction conditions is documented. Attributing systemic signs to “silicone sensitivity” without ruling out organotin exposure is a diagnostic gap that shows up repeatedly in occupational medicine case reviews.
| Silicone/Siloxane Species | Toxicity Classification | Primary Exposure Route | Key Regulatory Threshold |
|---|---|---|---|
| PDMS (high MW, ≥20,000 Da) | Practically non-toxic systemically | Dermal/ingestion (low absorption) | FDA 21 CFR 175.105 food-contact clearance |
| D4 (octamethylcyclotetrasiloxane) | SVHC; reproductive toxicant (Cat. 2) | Inhalation (vapor) | REACH Annex XIV; CA Prop 65 NSOEL 1,100 µg/day |
| D5 (decamethylcyclopentasiloxane) | PBT under REACH; endocrine scrutiny | Inhalation (vapor) | REACH SVHC; EU restriction in wash-off >0.1% w/w |
| D6 (dodecamethylcyclohexasiloxane) | Under REACH PBT review | Inhalation (vapor) | Parallel REACH review; no standalone WEL established |
| VTMO / APTES (alkoxysilanes) | Irritant; methanol/ethanol release on hydrolysis | Inhalation, skin/eye contact | MeOH OSHA PEL 200 ppm TWA; confirm SDS per grade |
| Chlorosilanes | Corrosive; acute HCl generation | Inhalation, skin/eye contact | OSHA PEL HCl 5 ppm ceiling; NIOSH REL 5 ppm |
| Organotin catalysts (DBTDL, DOTL) | Hepatotoxic; immunotoxic | Dermal, inhalation of vapors | No single WEL; ICP-OES detection at ppb in cured matrix |
Understanding this taxonomy is not academic. The hazard controls, medical surveillance markers, regulatory reporting obligations, and emergency response procedures are materially different for each species. A single SDS labeled “silicone elastomer” may require cross-referencing three separate regulatory frameworks before a plant safety team has an accurate picture of what they are actually managing.
Occupational Exposure Signs: Acute and Chronic Symptoms Mapped to Specific Silicone Compounds
Not every exposure event announces itself with an alarm. The more dangerous pattern in silicone-handling facilities is the worker who attributes a persistent headache to the afternoon heat, or the maintenance tech whose blood work comes back slightly off six weeks after a catalyst changeover — and neither event gets linked to the silicone line. Mapping symptoms to their actual causative species is the first operational step toward a defensible EHS response protocol.
Acute Respiratory Signs: Chlorosilanes and Silane Vapor
The fastest-moving hazard in silicone manufacturing is chlorosilane hydrolysis. When trichlorosilane, methyltrichlorosilane, or dimethyldichlorosilane contacts atmospheric moisture — including the humidity in a worker’s upper airway — it generates HCl instantaneously. Symptoms follow within two to five minutes of exposure above roughly 1 ppm HCl equivalent: lacrimation, rhinorrhea, and a characteristic sharp cough. Above 3–5 ppm, bronchospasm can develop, and workers with pre-existing reactive airway disease are disproportionately affected. The OSHA PEL for HCl is a 5 ppm ceiling — not a TWA — which means brief peak excursions during drum changes, hose disconnections, or reactor venting are the operationally relevant exposure events, not the steady-state floor concentration.
In a typical bulk chlorosilane transfer operation, a corroded quick-connect fitting leaks a small vapor pulse during coupling. The concentration spike lasts under 30 seconds, well below any alarm threshold on a fixed monitor calibrated for longer averaging periods. Workers compensate by turning their heads — and over weeks, a pattern of morning hoarseness and mild rhinitis gets attributed to seasonal allergies. The fix is NIOSH ceiling methodology monitoring at the breathing zone during coupling operations, not reliance on area monitors alone.
Dermal and Mucosal Signs: Uncured Formulations and Aminosilane Sensitization
Cured silicone elastomer is largely inert against skin. The hazard lives in the uncured formulation. Aminosilanes — 3-aminopropyltriethoxysilane (APTES) being the most common industrial example — are documented IgE-mediated sensitizers. First-exposure dermatitis may appear mild: erythema at contact sites, slight vesiculation at the wrist cuffs where gloves end. The clinical trap is distinguishing IgE-mediated allergic contact dermatitis from the irritant contact dermatitis caused by the organic solvents often present in the same formulation. The differentiation matters operationally: irritant dermatitis resolves when the solvent exposure stops; allergic sensitization does not, and re-exposure at even lower concentrations can trigger a full response.
Workers handling two-part RTV or condensation-cure systems often develop symptoms at the hands and forearms first. If the same worker rotates to a purely PDMS-based operation and symptoms persist, the aminosilane is the more likely culprit — not the base polymer.
Cured silicone rubber causes allergic contact dermatitis through direct skin contactFalse
Fully cured high-MW PDMS is essentially non-reactive at the skin surface. Allergic sensitization in silicone-handling workers is overwhelmingly traced to reactive species in uncured formulations — especially aminosilanes and residual crosslinkers — not to the cured polymer matrix itself.
Systemic Signs: D4/D5 Inhalation and Reproductive Concern
Cyclic siloxane vapors (D4, D5) are generated during silicone mixing, mold-release application, and high-shear compounding. Individual compound odor thresholds are low enough that workers may not reliably detect air concentrations approaching 10 ppm — the UK BOHS practical working reference for total siloxane vapor. At concentrations in this range, reported symptoms include headache, dizziness, and nausea, which operators commonly misattribute to poor ventilation generally rather than to a specific chemical species.
The chronic concern is more consequential and harder to observe in real time. D4 carries confirmed reproductive toxicity classification under REACH; D5 carries ongoing endocrine disruption scrutiny. Sub-threshold chronic exposures produce no acute symptom signal — which is precisely the risk. California Prop 65 lists D4 with a No Significant Exposure Level (NSOEL) for reproductive toxicity at 1,100 µg/day, a figure that translates to a surprisingly small air concentration when integrated over a full shift. Urinary dimethylsilanediol (DMSD) is the validated biomonitoring marker: unexposed individuals generally show below 2 µg/g creatinine; occupational exposure above threshold is flagged at roughly 20 µg/g creatinine. Periodic biomonitoring in D4/D5-handling roles gives EHS managers something measurable — reproductive concern stops being invisible.
Organotin Catalyst Signs: The Delayed Blood-Panel Pattern
Organotin compounds — dibutyltin dilaurate, stannous octoate — are standard condensation-cure catalysts and among the most underappreciated occupational hazards in the silicone processing chain. Their toxicity signature does not appear acutely. Workers present two to six weeks post-exposure with nonspecific fatigue, a depressed lymphocyte count on a routine CBC, and elevated ALT/AST on a metabolic panel. These findings rarely trigger a chemical exposure investigation on first presentation — they are more often attributed to viral illness or occupational stress.
The operational pattern that precedes the blood findings: catalyst drum changeovers performed without supplied-air respirators, relying on half-face cartridge respirators that are not rated for organotin vapor. Because the catalyst is used at low concentration and the immediate odor is faint, the exposure perception is low. EHS programs that do not specifically include organotin compounds in their respiratory protection program — treating them as a minor ancillary chemical — are the facilities where these delayed hepatic and immune findings appear most consistently.
Thermal Degradation Signs: The 200°C Processing Threshold
Silicone at ambient temperature is a minimal hazard. Silicone heated above 200°C in the presence of even trace acid or base catalyst begins generating formaldehyde and carbon monoxide as thermal depolymerization byproducts. Workers in curing ovens, post-cure operations, or silicone-coated substrate processing first present with eyes, nose, and throat irritation — the classic irritant triad. Formaldehyde carries an OSHA PEL of 0.75 ppm TWA and 2 ppm STEL; the irritant symptoms at or above the STEL are diagnostically useful early indicators that formaldehyde generation is occurring.
Above 450°C — silicone combustion — fine respirable crystalline silica particulate is generated. The exposure consequence is not acute; pulmonary fibrosis risk from respirable SiO2 accumulates over years of sub-threshold exposures, each below what would trigger an individual complaint. The OSHA respirable crystalline silica PEL of 0.05 mg/m³ applies directly. Facilities that periodically burn off silicone from mold tooling or incidentally combust silicone-contaminated scrap should be air-monitoring for respirable SiO2 — most are not.
Operational warning — the thermal processing drift: Processing temperature setpoints in ovens serving dual roles (silicone cure and other substrates) are frequently nudged upward over time to compensate for aging heating elements or to speed throughput. A setpoint that started at 180°C migrates to 220°C, then 240°C over 18 months — and a formaldehyde generation scenario that did not exist at commissioning is now running every shift. This is a classic “temporary becomes permanent” hazard: nobody made a single decision to accept the risk; it accumulated through small incremental adjustments, each individually minor.
Symptom-to-Compound Reference Table
| Observed Sign | Likely Causative Species | Exposure Threshold Reference | Recommended Immediate Action | Relevant Standard |
|---|---|---|---|---|
| Acute cough, lacrimation, rhinorrhea | HCl from chlorosilane hydrolysis | OSHA PEL: 5 ppm ceiling | Remove from area; medical evaluation if symptoms persist >30 min | OSHA 29 CFR 1910.1000 |
| Bronchospasm, chest tightness | HCl (high exposure event) | >5 ppm peak | Emergency medical response; spirometry follow-up | NIOSH REL: 5 ppm ceiling |
| Erythema, vesiculation at contact sites | Aminosilane (IgE-mediated) or formulation solvents | No established OEL; ACGIH TLV varies by compound | Patch testing to differentiate allergic vs. irritant; dermatology referral | ACGIH TLV documentation |
| Headache, dizziness, nausea | D4/D5 cyclic siloxane vapor | ~10 ppm working reference (BOHS) | Ventilation assessment; DMSD biomonitoring | UK BOHS guidance; no statutory WEL as of 2024 |
| Fatigue, lymphocyte depression, elevated ALT/AST | Organotin catalyst (DBT, DBTL) | No established OSHA PEL for most organotins | Targeted blood panel (CBC, LFTs); incident investigation of RPE compliance | REACH SVHC / ACGIH documentation |
| Eye/nose/throat irritation at oven operations | Formaldehyde (thermal depolymerization >200°C) | OSHA PEL: 0.75 ppm TWA / 2 ppm STEL | Air sampling; oven temperature audit; immediate engineering controls | OSHA 29 CFR 1910.1048 |
| Long-term pulmonary function decline | Respirable crystalline SiO₂ (combustion >450°C) | OSHA PEL: 0.05 mg/m³ | Silica air monitoring; baseline spirometry + annual follow-up | OSHA Silica Standard 29 CFR 1910.1053 |
Quick verdict: When a silicone-line worker presents with systemic fatigue and elevated liver enzymes 3–6 weeks after a process change, investigate the catalyst chemistry before the polymer.
Environmental Toxicity Indicators: How D4, D5, and D6 Signal Contamination in Plant Effluent and Supply Chain
Occupational exposure is visible — workers report symptoms, air monitors alarm, medical surveillance catches trends. Environmental contamination from cyclosiloxanes works on a different clock entirely. D4 and D5 don’t announce themselves in a discharge pipe; they accumulate quietly in biosolids, partition into sediment, and show up years later in regulatory audits, WWTP performance reports, or — in the worst trajectory — peer-reviewed literature documenting tissue concentrations in Arctic marine mammals. By the time a silicone processing facility faces permit scrutiny, the upstream procurement decisions that enabled that contamination are long forgotten. That gap between cause and consequence is precisely where supply chain liability lives.
D4 as a PBT Substance: The Long-Tail Liability Signal
D4 (octamethylcyclotetrasiloxane, CAS 556-67-2) carries a log Kow in the range of 7.6–8.0 — meaning it has an extreme preference for lipid phases over water. In practice, this translates to bioaccumulation in fatty tissues of aquatic and marine organisms even at low ambient water concentrations. Multiple peer-reviewed studies have documented D4 tissue concentrations in the range of 0.1–10 ng/g lipid weight in Arctic marine mammals, populations geographically remote from any silicone production site. The transport pathway runs through urban wastewater sludge applied to agricultural land, atmospheric deposition, and riverine discharge — all fed, at least partially, by industrial process water from silicone manufacturing and formulation.
For an environmental engineer at a silicone processing facility, the operational implication is direct: any process water stream containing PDMS polymer processing washouts, solvent rinses from silane coupling agent operations, or equipment cleaning condensate should be treated as a potential D4/D5 source. A grab sample showing D4 above 0.01 mg/L in pre-treatment effluent is not a minor housekeeping issue — it is a PBT release event with multi-year liability implications under both EU REACH Annex XIV and Canada’s CEPA virtual elimination policy for D4.
Persistent bioaccumulators don’t give you a second chance to act early. D4’s half-life in freshwater sediment commonly exceeds 100 days under low-turbulence, anaerobic conditions. A spill or chronic low-level discharge that appears resolved at the surface may continue leaching from settled solids for years.
WWTP Disruption: D5 as a Biological Treatment Inhibitor
D5 (decamethylcyclopentasiloxane, CAS 541-02-6) creates a different problem downstream — not bioaccumulation in the immediate effluent receiver, but disruption of the biological treatment process itself. D5 inhibits nitrifying bacteria (the ammonia-oxidizing organisms critical to biological nitrogen removal) at concentrations with an EC50 commonly reported in the range of 0.05–0.3 mg/L depending on bacterial strain and operating conditions. In operational terms: if a facility’s process water contains D5 above roughly 0.1 mg/L entering the aeration basin, nitrification efficiency degrades, effluent ammonia rises, and the plant begins violating its discharge permit — not because of the siloxane directly, but because the siloxane has killed the microbiology doing the compliance work.
In a typical specialty coatings plant running three shifts with batch solvent-cleaning of silicone-coated tooling, the D5 loading to the internal WWTP can spike significantly during shift changeover washdowns. Operators often compensate for rising effluent ammonia by increasing aeration or adjusting retention time — treating the symptom without identifying the siloxane source. The WWTP’s biological stage may remain partially impaired for weeks before anyone connects the chemistry.
Air Emission Monitoring and Community Air Quality Triggers
Atmospheric D4 monitoring near production facilities becomes a permit and community relations issue at concentrations approaching 0.1 µg/m³ in ambient community air — a level that regulatory agencies in several EU jurisdictions have used as a trigger threshold for further site investigation. Odor complaints from nearby residents are often the first operational signal, preceding any formal air quality measurement, because D4 has a recognizable slightly sweet, oily odor detectable by some individuals at concentrations well below acute health thresholds.
Facility air emission controls for D4/D5 are therefore not solely a worker protection measure — they directly affect site operating permits. Carbon adsorption units on oven exhaust streams handling silicone-coated substrates, condensate recovery on mixing vessel vents, and covered transfer operations are the practical engineering controls that keep ambient air concentrations in compliance and prevent the regulatory visibility that draws inspection attention.
Supply Chain Traceability: The 0.1% w/w Threshold and Procurement Obligations
EU REACH Annex XIV placed D4 under authorization requirements since 2018, and the restriction on D4/D5 in wash-off consumer products above 0.1% w/w has a direct supply chain traceability consequence that extends well upstream of consumer product formulators. Under REACH’s SVHC article notification obligation, the same 0.1% w/w concentration threshold triggers a supplier notification requirement down the supply chain for articles. A silicone polymer lot with poorly controlled cyclosiloxane residuals — not uncommon in lower-grade PDMS produced without post-stripping — can carry D4+D5+D6 totals in the range of hundreds to several thousand ppm depending on production process and purification depth.
If your raw material supplier cannot provide a Certificate of Analysis with quantified cyclosiloxane residuals (D3 through D6 at minimum), tested by GC-MS headspace analysis with detection limits in the 1–10 ppm range, you as the downstream processor carry the compliance burden if your finished product or article is found non-conforming. This is not a theoretical risk — EU market surveillance has tested formulated products and traced non-conformance back through supply chains, triggering corrective action obligations on processors who purchased non-conforming inputs in good faith.
Quick verdict: Specify maximum total cyclosiloxanes (D4+D5+D6) contractually — commonly ≤500 ppm total for industrial polymer applications, lower for wash-off or skin-contact formulations — and require GC-MS headspace data with each production lot, not just per specification sheet.
All food-grade or FDA-cleared silicone materials are automatically compliant with EU REACH D4/D5 restrictionsFalse
FDA 21 CFR 175.105 clearance for food-contact PDMS does not address cyclosiloxane residual content under EU REACH. A PDMS meeting FDA food-contact requirements can still contain D4 or D5 residuals above the 0.1% w/w REACH restriction threshold, requiring separate testing and documentation for EU market access.
ESG Reporting and Scope 3 Disclosure Pressure
In the US, D4 and D5 qualify for Toxics Release Inventory (TRI) reporting under EPCRA Section 313 when manufactured, processed, or otherwise used above threshold quantities (generally 25,000 lb/year processed or 10,000 lb/year otherwise used). EU PRTR (Pollutant Release and Transfer Register) and Japan’s PRTR scheme have equivalent reporting obligations. For industrial buyers with published Scope 3 emissions and chemical footprint commitments — increasingly a procurement qualification criterion in automotive, electronics, and personal care supply chains — a silicone supplier without PRTR/TRI reporting history, or with a history of reported releases trending upward, is a supplier whose ESG disclosures create downstream audit exposure.

| Siloxane Species | Environmental Fate Parameter | Regulatory Threshold / Trigger | Detection Method | Procurement Control Point |
|---|---|---|---|---|
| D4 | Log Kow ~7.6–8.0; PBT under EU REACH; sediment half-life >100 days (anaerobic) | REACH Annex XIV authorization required; Canada CEPA virtual elimination; EU wash-off restriction >0.1% w/w | GC-MS headspace (polymer matrix, LOD ~1–10 ppm); water: SPME-GC-MS | Require D4 residual data per lot; contractual cap ≤500 ppm (adjust down for wash-off/skin-contact use) |
| D5 | Log Kow ~8.03; classified PBT; WWTP nitrifier EC50 ~0.05–0.3 mg/L | EU wash-off restriction >0.1% w/w; ongoing endocrine disruption review | GC-MS headspace; liquid-liquid extraction for wastewater | Include D5 in SDS residual declaration; audit supplier WWTP compliance records |
| D6 | Log Kow ~8.8 (estimated); less regulated but co-elutes in cyclosiloxane burden | No standalone restriction as of 2024, but included in total cyclosiloxane contract specs | GC-MS headspace (co-quantified with D4/D5 in total siloxane method) | Specify D3–D6 total in QA clause; request third-party testing if supplier data is absent |
| D4/D5 (air) | Atmospheric transport; community odor and permit trigger | ~0.1 µg/m³ community ambient monitoring trigger (EU jurisdiction reference) | Atmospheric GC-MS; Tenax tube sampling | Request site emission monitoring reports for production facilities; flag odor complaint history |
| D4/D5 (WWTP sludge) | Partitions to biosolids; land application vector for bioaccumulation | Sludge quality criteria vary by jurisdiction; PBT status drives precautionary limits | Soxhlet extraction + GC-MS for solids | Ask supplier for WWTP sludge disposal method and D4/D5 characterization data |
Product Contamination and End-Use Failure as a Toxicity Signal: When the Part Tells You Something Is Wrong
Worker symptoms get the attention. Product failures get the production halt. In practice, silicone-related toxicity signals often appear first at the part level — a delaminating circuit board, a failed biocompatibility submission, a drug batch flagged for unidentified impurities — well before any occupational health report is filed. Quality engineers who recognize these downstream failure modes as chemical contamination indicators, rather than random process noise, gain weeks of diagnostic lead time.

Siloxane Outgassing and Adhesion Failure in Electronics Manufacturing
Surface energy collapse is one of the quietest, costliest failure modes in electronics assembly. When cyclosiloxane vapors — primarily D4 and D5 — deposit on treated substrates, they form a monolayer film that drives contact angle above 70° on surfaces engineered to accept adhesive bonding. At that threshold, solder mask adhesion, underfill wetting, and conformal coating adhesion all degrade measurably. The insidious part: the contamination is invisible, the silicone component responsible may be located meters away, and the assembly process reports nothing abnormal.
This mechanism has been documented at ambient D4+D5 vapor concentrations as low as 0.1 ppm in cleanroom air — well below any occupational concern threshold, but sufficient to passivate a gold bondpad or a pre-cleaned PCB surface within hours of exposure. Operators often compensate by increasing plasma-cleaning frequency or adjusting adhesive formulations, neither of which addresses the source.
In a typical high-density PCB assembly environment, silicone-insulated wire harnesses stored near open component trays introduce enough outgassing to measurably degrade surface energy on boards staged overnight. The fix is segregated storage with clean-room-grade polyethylene containment — not a process change upstream.
Quick verdict: If contact-angle measurements on freshly cleaned substrates are drifting upward over weeks without a documented process change, treat it as a siloxane outgassing audit trigger before suspecting cleaning chemistry.
Medical Device Extractables: ISO 10993-13 as the Formal Detection Framework
For implant-grade silicone, the formal signal pathway runs through extractables/leachables testing under ISO 10993-13. Uncured silicone oligomers — low-MW cyclosiloxanes and short linear chains — migrate from the polymer matrix into adjacent tissues or drug-contact fluids. The approximate working threshold for Class III implants is extractable siloxane exceeding 10 µg per device, at which point a full biological evaluation is triggered rather than a reliance on material equivalence.
The practical implication for procurement: a certificate of conformance that declares “medical-grade silicone” without a volatile content specification and a cyclosiloxane assay result is not fit for Class III supply chain documentation. The CoA line items that actually correlate with biological risk are: residual catalyst concentration (platinum complex carryover), cyclosiloxane content by GC-MS headspace (D4 through D6 individually), and Shore A hardness as a proxy for cure completeness.
FDA food-contact clearance under 21 CFR 175.105 means high-MW PDMS presents no extractables risk in medical applicationsFalse
FDA 21 CFR 175.105 addresses food-contact use of high-molecular-weight PDMS — it is not a biological safety declaration. Extractables/leachables risk in medical devices is evaluated under ISO 10993-13, which requires compound-specific quantification of migrating oligomers regardless of bulk polymer grade.
Food Contact and Pharmaceutical Signals: Temperature-Driven Migration
Silicone bakeware and gaskets used above 175°C release cyclosiloxanes into food simulants at rates that scale with temperature and surface-area-to-volume ratio. Under the EU Regulation 10/2011 migration limit framework, specific migration limits (SMLs) apply, and the first consumer-facing indicator is almost always organoleptic: an off-odor or taste taint in the food product, typically described as waxy or slightly chemical, before any analytical flag is raised.
In pharmaceutical manufacturing, silicone tubing used in peristaltic pump systems leaches D4 and D5 into drug product at sub-ppm concentrations detectable by GC-MS headspace analysis. This sits in the same analytical and regulatory territory as ICH Q3C residual solvent guidance — the question is not whether leaching occurs, but whether the leached quantity crosses the threshold that requires characterization and patient risk assessment. FDA warning letters have cited siloxane contamination in injectable drug manufacturing, specifically in contexts where tubing was used beyond validated service intervals or where compression set had advanced enough to increase surface contact and diffusion.
Coatings and Sealants: FTIR as the Forensic Language
Cured silicone sealant failure — yellowing, surface tack loss, or cohesive splitting — is typically attributed to UV exposure or substrate movement. The more chemically specific diagnosis requires FTIR. Oxidative degradation and catalyst poisoning share a forensic signature: attenuation of the Si–CH₃ symmetric deformation peak at 1260 cm⁻¹ paired with the emergence of broad Si–OH absorption between 3200 and 3700 cm⁻¹. That pattern indicates methyl group loss and chain scission, not simply weathering.
Operational warning — the “temporary becomes permanent” failure path: In construction and industrial sealing, a sealant showing early tack loss is frequently overcoated rather than replaced. The Si–OH accumulation beneath the overcoat continues. By the time cohesive failure becomes visible, water ingress has been occurring for months. The sealant has been signaling chemical degradation the whole time; the forensic signal was simply never read.
Incoming Inspection Protocol: Catching the Signal Before It Enters Production
| Application Sector | Observable Failure Mode | Underlying Chemical Signal | Test Method | Specification Limit (typical working range) |
|---|---|---|---|---|
| Electronics / PCB assembly | Adhesion failure, delamination, contact-angle rise | D4+D5 surface deposition from outgassing | Contact-angle goniometry; GC-MS headspace of nearby silicone components | Contact angle ≤70° on treated substrate; D4+D5 vapor <0.1 ppm in cleanroom zone |
| Medical devices (Class III) | Failed biocompatibility submission, implant reactivity | Extractable cyclosiloxane oligomers | ISO 10993-13 extractables/leachables; GC-MS headspace | Extractable siloxane 5 ppm (50% of 10 ppm BOHS reference) | Industrial Hygienist | Monitoring log, corrective action record |
| Surface wipe (dermal) | Hexane wipe + GC-MS | >1 µg/cm² on skin-contact surfaces | EHS Technician | Wipe sampling report, glove protocol update |
| Biological monitoring | Urinary DMSD (spot or end-of-shift) | >20 µg/g creatinine | Occupational Physician | Medical surveillance record (confidential) |
| Medical surveillance | LFT panel; spirometry; reproductive health review | As clinically indicated per exposure history | Occupational Physician | Annual surveillance report |
| Supplier CoA review | CAS-level oligomer limit vs. CoA data | Any cyclic siloxane >0.1% w/w undisclosed | Procurement / EHS Lead | Non-conformance record, SDS accuracy log |
Audit scope creep is a real risk: facilities commonly restrict air sampling to primary processing areas and miss secondary exposure zones — maintenance bays where cured silicone is cut or ground, waste handling areas, and HVAC return paths that concentrate volatiles from multiple upstream sources. A silicone toxicity audit that only covers the production floor is incomplete by design.
Thermal Degradation and Processing Hazards: The Hidden Toxicity Window in Silicone Manufacturing and Fabrication
Most occupational exposure incidents with silicone don’t happen during storage or handling of raw polymer — they happen inside ovens, at mold faces, and along curing lines where engineers are focused on process yield, not vapor chemistry. Thermal degradation is the mechanism that transforms a largely inert bulk material into a cocktail of reactive small molecules, and the hazard profile shifts dramatically across a span of fewer than 300°C. Getting the temperature thresholds right isn’t academic; it’s the difference between a well-controlled cure cycle and a shift of workers going home with splitting headaches that nobody can explain until the third incident.
Three Distinct Processing Risk Zones
PDMS and related methylsiloxane polymers don’t degrade in a single step. The hazard escalates in recognizable stages:
Below 150°C: In the absence of catalytic contamination, thermal volatilization is the dominant mechanism. Residual low-molecular-weight cyclosiloxanes — primarily D4 and D5 — migrate to the surface and volatilize. No significant chain scission. Toxicity risk is primarily cyclosiloxane inhalation exposure, manageable with general ventilation if concentrations are modest. The danger here is complacency: operators often assume that because nothing is visibly smoking, nothing hazardous is present.
150–250°C: This is the zone where processing risk becomes genuinely complex. Two things happen simultaneously. First, if trace acid or base catalyst is present — residual from cure chemistry, from a contaminated mold release, or from equipment cleaning agents — PDMS depolymerization to cyclic oligomers accelerates sharply, with measurable onset above approximately 150°C under catalyzed conditions. Second, and less widely recognized, methylsiloxane oxidation in this temperature range generates formaldehyde. The OSHA PEL for formaldehyde is 0.75 ppm TWA with a 2 ppm STEL — and formaldehyde monitoring is routinely absent from silicone processing facilities that have never been flagged for it. LSR injection molding at standard mold temperatures of 170–200°C and silicone resin oven-cure coating lines running 120–180°C both sit inside this window.
250–350°C: Uncatalyzed thermal depolymerization becomes significant. Cyclosiloxane vapor concentrations rise steeply. Any residual peroxide curing agents decompose, adding organic byproducts to the vapor stream. Steam autoclave vulcanization of silicone gaskets can push local temperatures into this range during pressure excursions, and the combination of heat, moisture, and residual catalyst creates an environment where the degradation product profile is genuinely difficult to predict without sampling.
Above 450°C: Combustion. The dominant solid product is amorphous SiO₂ fume at nanoscale particle sizes. This is not the same as respirable crystalline silica regulated at the OSHA PEL of 0.05 mg/m³, but it carries its own respiratory hazard: amorphous silica in certain forms is classified IARC Group 2A, and ultrafine particles drive pulmonary inflammatory response by surface-area-driven mechanisms rather than crystal-structure toxicity. Carbon monoxide is also generated. Any silicone fire, or any process that allows localized overheating to combustion temperatures, must be treated as a combined CO and silica-fume event.
| Process Temperature Range | Dominant Degradation Product | Toxicity Classification | Monitoring Method | Engineering Control |
|---|---|---|---|---|
| 450°C | Amorphous SiO₂ fume; CO | Pulmonary inflammation (amorphous silica); CO asphyxiation | Real-time CO monitor; respirable dust gravimetry | Emergency ventilation; CO alarm; SCBA access |
Ventilation Engineering: Where Most Facilities Fall Short
The ACGIH Industrial Ventilation Manual specifies a minimum LEV capture velocity of 0.5–1.0 m/s at open-surface oven and tank operations — the lower end for low-toxicity materials, the upper end where formaldehyde or reactive species are involved. In practice, many silicone curing lines rely on dilution ventilation: general room air changes rather than source capture. For high-vapor-pressure silane operations or any process above 200°C, dilution ventilation alone is inadequate. The math is unforgiving: dilution ventilation manages low-release-rate background contamination; it cannot reliably control a burst emission at oven door opening when ten square meters of freshly cured part surface flashes vapor into the operator’s breathing zone.
Operational warning — the formaldehyde blind spot: Facilities that have passed siloxane air monitoring without incident often have never tested for formaldehyde co-generation during silicone oven cure. The two hazards require different detector technologies. A photoionization detector calibrated for cyclosiloxane will not reliably flag formaldehyde at the OSHA PEL. If your monitoring program doesn’t include an electrochemical formaldehyde sensor at curing oven face height, the exposure data you have is incomplete.
Recognizing the Aggregate Symptom Pattern
In a typical high-throughput silicone coating operation — running a resin-based product at 230–250°C through a continuous belt oven without local exhaust — the incident pattern tends to emerge not as a single acute event but as a cluster: multiple workers on the same shift reporting headaches and mild nausea by the third hour, with a respiratory irritation component that operators initially attribute to “the smell of the cure.” Root-cause investigation, when it finally happens, typically finds formaldehyde at 0.8–1.4 ppm at breathing zone height near the oven exit, well above the OSHA PEL, alongside D4/D5 concentrations that individually seem marginal but create an additive irritant burden. The common mistake is investigating the two hazards independently when they are co-generated and co-experienced. The fix is simultaneous multi-analyte monitoring and LEV engineering at oven exit, not just at the infeed.
Silicone is non-toxic at all processing temperatures because it is an inert polymerFalse
Bulk high-MW PDMS is chemically stable at ambient conditions, but thermal processing above 150°C with trace catalysts generates cyclosiloxane vapors and formaldehyde. Above 450°C, combustion produces amorphous SiO₂ fume and CO. Inertness is temperature-dependent and catalyst-dependent, not absolute.
Quick verdict: If your silicone processing temperature exceeds 180°C and formaldehyde is not on your air-monitoring panel, your industrial hygiene program has a gap — regardless of how long the line has run without a reported incident.
Regulatory Thresholds and Global Classification Landscape: What Procurement and Compliance Teams Must Reconcile
The regulatory map for silicone-related substances is not a single document — it is a patchwork of overlapping jurisdictional regimes that classify the same molecule differently, set different disclosure triggers, and assign different supply-chain obligations depending on where the finished product lands. Procurement teams that rely on a single global SDS are almost certainly non-compliant somewhere. The practical consequence is not just a fine; it is a shipment held at customs, a customer audit failure, or a reformulation demand that arrives six weeks before a product launch.
EU REACH: The Strictest Regime for D4 and D5
Under EU REACH, D4 (octamethylcyclotetrasiloxane, CAS 556-67-2) has been on Annex XIV — the Authorization List — since 2018. Any substance or formulation containing D4 above 0.1% w/w that is placed on the EU market in wash-off cosmetic products is subject to restriction, and any industrial use requiring authorization must demonstrate no suitable alternatives or obtain a specific use authorization from ECHA. For importers of silicone fluids or formulations sourced from outside the EU, residual D4 in the polymer matrix is not a theoretical concern; it is a measurable assay requirement. GC-MS headspace analysis routinely detects D4 at 1–10 ppm in polymer matrices, and many commercial PDMS grades carry residuals in that band without explicit supplier declaration.
D5 (decamethylcyclopentasiloxane, CAS 541-02-6) carries a log Kow of 8.03 and a PBT classification under REACH, with ongoing restriction evaluation in personal care and industrial contexts. Its SVHC status means the 0.1% w/w threshold in articles triggers a mandatory supplier notification obligation down the supply chain — a requirement that catches distributors and compounders who assume only the original formulator bears the burden.
A single global SDS covers REACH, TSCA, and CEPA compliance for silicone formulations containing D4 or D5False
Each jurisdiction imposes different classification status, concentration thresholds, disclosure triggers, and labeling requirements for D4 and D5. A single SDS cannot satisfy all three simultaneously without jurisdiction-specific addenda.
US Federal and California: A Split Regulatory Posture
At the federal level, D4 and D5 are not currently on the TSCA High Priority Substances list, but both are subject to Significant New Use Rules (SNURs) in defined application contexts, meaning a change in use pattern can trigger EPA review without any new toxicity finding. The practical implication for formulators introducing silicone-containing products into new industrial applications is that a use-change analysis is not optional paperwork; it is a legal prerequisite.
California Prop 65 introduces a reproductive toxicity dimension. The no-observed-effect level for D4 is established at 1,100 µg/day — a figure that matters most for consumer-adjacent industrial products like mold-release agents, coatings, or maintenance aerosols used in food-processing environments, where incidental ingestion pathways cannot be dismissed.
Canada: The Strictest Jurisdictional Stance
Canada’s CEPA 1999 assessment designated D4 as toxic under Schedule 1, triggering a virtual elimination policy for environmental releases. This is materially stricter than the US federal position and requires suppliers exporting formulations into Canada to provide explicit D4 content disclosure — not merely an SDS flag. In a typical multi-tier supply chain where a Chinese silicone polymer manufacturer sells to a European compounder who sells to a Canadian industrial customer, the D4 assay data must survive all three handoffs intact. It commonly does not, which is why Canadian importers are increasingly issuing supplier questionnaires that demand GC-MS certificates of analysis rather than accepting a generic low-hazard classification.
China and Japan: Gaps and Emerging Requirements
China’s GB/T 23947 covers industrial silicone fluid specifications, and GBZ 2.1 sets occupational exposure limits for relevant silanes. Critically, China’s OEL framework does not yet include specific cyclosiloxane TWA limits for D4 or D5. For exporters manufacturing in China and selling into regulated markets, this creates a compliance asymmetry: the production environment may be technically within Chinese domestic requirements while the exported product triggers REACH or CEPA disclosure obligations that the domestic OEL framework does not prompt.
Japan’s PRTR law designates D4 as a Class I Designated Chemical Substance, requiring facilities above a threshold quantity to report annual release and transfer data. Japan’s Industrial Safety and Health Law (ISHL) provides technical guidance on silane handling — particularly relevant for semiconductor fab operations where chlorosilane precursors and cyclosiloxane byproducts coexist in the same process train.

Compliance Matrix: What Supplier Data Points Each Jurisdiction Requires
| Jurisdiction | Regulated Species | Classification Status | Key Threshold / Limit | Supplier Disclosure Requirement |
|---|---|---|---|---|
| EU (REACH) | D4, D5 | D4: Annex XIV; D5: PBT/SVHC | 0.1% w/w in articles/formulations | SVHC notification; Annex XIV authorization for D4 uses |
| US Federal (TSCA) | D4, D5 | Not High Priority; SNUR-applicable | Use-specific; no blanket TWA limit | SNUR notification if new use introduced |
| US California (Prop 65) | D4 | Reproductive toxicant listed | NSOEL 1,100 µg/day | Warning label if exposure exceeds NSOEL |
| Canada (CEPA) | D4 | Schedule 1 — toxic | Virtual elimination for environmental release | Explicit content disclosure; GC-MS CoA recommended |
| China (GB/GBZ) | Relevant silanes | OEL framework; no D4/D5 TWA | No cyclosiloxane-specific TWA established | Domestic OEL compliance; export destinations set additional requirements |
| Japan (PRTR/ISHL) | D4 | Class I Designated Chemical | PRTR reporting threshold (annual release/transfer) | Annual facility reporting above quantity threshold |
Quick verdict: If your supplier cannot provide a GC-MS certificate of analysis for D4 and D5 residuals by lot, their SDS alone cannot demonstrate multi-jurisdictional compliance — build the assay requirement into your purchase specification, not your incoming inspection.
The operative risk for procurement teams is not which jurisdiction is strictest in isolation; it is that the same silicone formulation shipped to three different markets requires three different documentation packages, and the cost of getting it wrong scales with the destination. EU customs holds on SVHC-non-compliant articles can run weeks; Canadian regulatory action on undisclosed Schedule 1 substances carries both civil and director-level liability under CEPA’s enforcement provisions.
Hidden Cost Framework: How Unmanaged Silicone Toxicity Risk Translates Into Quantifiable Business Loss
Most facilities treat silicone toxicity management as a compliance cost — a line item to minimize. That framing inverts the actual economics. The real question isn’t what monitoring costs; it’s what an unmanaged incident costs relative to what prevention costs. At industrial scale, those two numbers are separated by one to three orders of magnitude.

Worker Illness Claims vs. Industrial Hygiene Monitoring
The US BLS proxy data for occupational illness claims in chemical manufacturing puts individual claim costs in the range of $40,000–$150,000 per claim, depending on severity, duration of treatment, and whether litigation follows. That range covers direct medical costs, workers’ compensation premiums, lost-time replacement labor, and administrative burden — it does not capture the long-tail productivity drag when an experienced process operator leaves a role due to a chronic respiratory condition that took two years to attribute.
A mid-size facility running silicone compounding or chlorosilane-adjacent processes can implement a credible annual industrial hygiene monitoring program — personal air sampling, biological exposure index tracking including urinary DMSD, ventilation performance verification — for somewhere in the range of $8,000–$25,000 per year depending on facility size, compound mix, and the number of monitored workers. One claim at the low end of the BLS range erases roughly two to three years of that investment. One claim at the high end erases a decade.
The math is straightforward. The decision to underinvest rarely is. Monitoring programs get deferred because they produce no visible output when everything is fine — which is precisely when they are working.
Regulatory Fine Exposure Across Jurisdictions
EU REACH non-compliance penalties for placing restricted substances on the market are set at the member-state level and range from approximately €10,000 for minor documentation failures to €500,000 or above for deliberate or repeat violations involving Annex XIV restricted substances such as D4. An OSHA willful violation in the US for silane handling failures — inadequate LEV, missing SDS, no respiratory protection program — carries a maximum penalty of $156,259 per violation as of 2024 inflation-adjusted figures. Those fines are per violation, not per incident, which means a single audit finding multiple deficiencies multiplies quickly.
EU REACH penalties for siloxane non-compliance are uniform across all member statesFalse
REACH sets the framework obligation but enforcement and penalty levels are implemented at the member-state level, meaning penalty severity varies significantly across the EU — a supplier's compliance exposure depends heavily on which national authority conducts the inspection.
Product Recall and Supply Chain Disruption
Consider a typical pharmaceutical contract manufacturer using silicone gaskets in a batch reactor system. If cyclosiloxane extractables from an unqualified gasket lot exceed the ISO 10993-13 working threshold for a Class III device equivalent, or migrate into a drug product at detectable levels, the recall scenario becomes plausible fast. Recall costs in pharmaceutical contexts commonly range from $1M to $10M once product destruction, FDA notification, customer remediation, and batch rework costs are consolidated. A GC-MS headspace test for cyclosiloxane content on an incoming gasket lot runs $200–$800 per lot. The cost ratio is not ambiguous.
Supply disruption carries its own arithmetic. When a silicone polymer supplier loses REACH authorization status mid-contract, qualifying an alternate supplier typically takes 6–12 weeks under normal conditions — longer if the formulation requires re-validation. For a mid-volume manufacturer, production downtime in that window commonly runs $50,000–$200,000 per week depending on line configuration and order backlog. Supplier qualification audits that include REACH substance management cost a fraction of one week’s downtime.
ESG and Reputation Costs: The Slow Financial Bleed
Undisclosed D4 or D5 content in formulations supplied into sustainability-audited supply chains has triggered customer delisting events — quietly, without litigation, simply as a procurement decision made during an EcoVadis or CDP review cycle. Those revenue losses don’t appear in incident reports. They appear as lost contract renewals attributed to “strategic sourcing realignment.”
The Cost-Benefit Inversion Table
The core financial logic: total addressable risk (TAR) equals the probability-weighted sum of incident costs. A 1% annual probability of a $500,000 event has an expected annual cost of $5,000. Any prevention spend below that level generates positive expected ROI. Most facilities are underinvesting because they anchor on the prevention cost as a certain outflow and discount the incident cost as unlikely. The probability estimate is usually wrong in the wrong direction.
| Risk Category | Annual Probability Range | Cost if Unmanaged | Annual Prevention Cost | ROI Ratio (approx.) |
|---|---|---|---|---|
| Worker occupational illness claim | 2–8% per exposed worker | $40,000–$150,000 per claim | $8,000–$25,000 (IH program) | 3:1 to 15:1 |
| Regulatory fine (REACH / OSHA) | 5–15% if non-compliant | €10,000–€500,000 / $156,259 per violation | $3,000–$10,000 (compliance audit) | 5:1 to 50:1 | |
| Product recall (pharma / medical) | 1–5% per unqualified lot | $1,000,000–$10,000,000 | $200–$800 per lot (GC-MS testing) | 100:1 to 1,000:1 |
| Supply chain disruption | 3–10% annually if single-sourced | $50,000–$200,000/week downtime | $5,000–$15,000 (supplier audit) | 10:1 to 100:1 |
| ESG / customer delisting | 2–10% over 3-year horizon | $100,000–$2,000,000 (lost contract value) | $2,000–$8,000 (supply chain disclosure) | 15:1 to 80:1 |
The probability ranges are illustrative order-of-magnitude estimates; actual facility risk depends on compound exposure profile, process configuration, regulatory jurisdiction, and supply chain structure. What the table makes visible is that even conservative probability assumptions produce positive prevention ROI across every risk category — and that the recall row, in particular, makes silicone lot testing one of the highest-return quality investments available in materials procurement.
Operational warning: The “temporary becomes permanent” cost trap. Many facilities run unvalidated silicone grades sourced during a supply emergency — and never requalify them. The original specification gets quietly retired because the line kept running. Cyclosiloxane content, cure chemistry, and extractable profiles in substitute grades are often unknown. This is not a hypothetical; it is a recurring finding in supplier audits. The cost of requalifying a substitute grade runs $5,000–$20,000. The cost of discovering the problem during a customer audit or recall investigation runs orders of magnitude higher.
Shop-Floor Voice FAQ: Questions Process Engineers and EHS Technicians Actually Ask About Silicone Toxicity

Our workers mix two-part silicone sealant all day with no symptoms — does that mean it’s safe?
Not quite, and this is one of the most common misreads in industrial silicone handling. Cured PDMS is genuinely low-hazard — the concern is what’s in the uncured system. Part B catalysts in addition-cure systems frequently contain organotin compounds (dibutyltin dilaurate is common), and condensation-cure systems may carry residual cyclosiloxanes — primarily D4 and D5 — in the Part A base. Neither produces the kind of acute irritation that triggers a complaint. The risk is chronic and subclinical: organotin accumulation affecting liver function, and cyclosiloxane reproductive effects that build over months of daily exposure. Absence of symptoms is not clearance. The correct monitoring protocol is periodic urinary dimethylsilanediol (DMSD) — an unexposed reference is below 2 µg/g creatinine, with occupational concern rising above roughly 20 µg/g creatinine — paired with a liver function panel for workers with sustained Part B contact. If your operation runs three shifts with continuous mixing, annual biological monitoring is the minimum defensible interval.
We heated a silicone gasket to 300°C during a process trial and workers complained of headaches — is that silicone toxicity?
Headaches at 300°C are almost certainly formaldehyde and carbon monoxide, not the silicone polymer itself. PDMS thermal depolymerization under uncatalyzed conditions begins around 300°C, and one of the degradation products in the presence of residual organic additives is formaldehyde — OSHA’s TWA PEL is 0.75 ppm, with a 2 ppm STEL. CO can accumulate rapidly in confined areas where combustion is incomplete. Your first response action is direct-reading CO monitoring and formaldehyde dosimetry badges on the workers nearest the heat source, not a silicone toxicity workup. If the gasket contained any acid or base catalyst residue, depolymerization onset drops to around 150°C, which means 300°C is well inside an active degradation window. Review whether the process temperature was intentional or a runaway, and check local exhaust ventilation capture velocity against the ACGIH benchmark of 0.5–1.0 m/s for oven operations.
Our CoA shows less than 0.1% volatiles — does that mean no D4/D5 risk?
No. Total volatile content on a CoA is a bulk mass-loss figure, typically measured by weight after oven aging. It does not differentiate between water, short-chain linear siloxanes, D3, D4, D5, and D6. A material could show 0.08% total volatiles and still carry a meaningful cyclosiloxane fraction if D4 and D5 represent most of that volatile fraction. For a compliance-grade answer — particularly relevant for EU REACH Annex XIV, wash-off product restrictions, or ISO 10993-13 extractables work — you need a dedicated GC-MS headspace assay that reports D3 through D6 individually. Detection limits in a well-configured lab run 1–10 ppm depending on sample preparation. Request this analysis explicitly from your supplier; a standard CoA will not give it to you.
A CoA showing less than 0.1% total volatiles confirms a product is free of restricted cyclosiloxanes.False
Total volatile content is a gravimetric bulk measurement and does not speciate cyclosiloxane fractions. Confirming D4/D5 status requires a dedicated GC-MS assay reporting D3–D6 individually.
Is there a safe exposure level for D4 in the workplace?
There is no established federal TWA OEL for D4 in the United States — OSHA has not promulgated one, and NIOSH has not issued a REL specific to D4. The most operationally useful reference is the UK BOHS practical guidance of 10 ppm as a working benchmark for total siloxane vapor, which many US-based industrial hygienists adopt by default. Reproductive toxicity is the primary driver of concern — California Prop 65 lists a No Significant Occupational Exposure Level (NSOEL) for D4 at 1,100 µg/day. In practice, responsible EHS programs set an internal action level of 5 ppm, triggering enhanced ventilation review and biological monitoring. The absence of a federal OEL is not a green light; it reflects regulatory lag, not a clean toxicology record.
We switched silicone suppliers and workers started reporting skin irritation within two weeks — where do we start?
Supplier transitions are a classic trigger that plants underweight. Start systematically: request the full SDS and CoA from the new supplier and compare catalyst type and loading against your previous source. The most common culprit in irritation complaints is an aminosilane crosslinker — amino-functional silanes are skin sensitizers at concentrations that don’t always generate an obvious smell. Check whether the new formulation uses a different cure chemistry (condensation vs. addition) that could mean a different residual profile. Run an FTIR scan of the new material against your retained sample of the old material — a shifted carbonyl peak or a new amine absorption band will point you toward the chemistry change quickly. For affected workers, a standard occupational dermatology patch-test protocol distinguishes irritant contact dermatitis from sensitization, which matters because sensitized workers cannot return to exposure without risk of escalating reactions.
Does “food-grade” or “pharmaceutical-grade” silicone mean zero toxicity risk at our process conditions?
Grade designations are compliance labels, not toxicology clearances — and process engineers conflate the two more often than they should. FDA 21 CFR 175.105 clearance for food-contact PDMS, for example, is granted based on specific migration testing at defined temperatures and with defined food simulants. If your process runs hotter than the test conditions, or contacts a food matrix with a higher fat content than the simulant used, cyclosiloxane migration can exceed the basis on which the clearance was issued. Similarly, ISO 10993-13 extractables thresholds for medical-grade silicone components are device-class and geometry-specific — a Class III implant triggers concern above approximately 10 µg extractable siloxane per device, and that threshold was derived under specific extraction protocols. In a typical pharmaceutical packaging operation, a “pharma-grade” silicone tubing that passes specification testing at 25°C may generate a different extractable profile at 80°C sterilization temperatures. Always validate at actual process conditions, not at the grade label’s baseline test parameters.
Supplier Qualification and Procurement Specification: Translating Toxicity Knowledge Into Enforceable Buying Standards
Knowing the toxicology is necessary. Putting it in the purchase order is what actually protects your plant, your product, and your liability position. Most of the occupational and product-contamination failures described in earlier sections trace back not to ignorance of the hazards but to procurement documents that never converted that knowledge into a testable, enforceable standard — and suppliers who were never asked to prove compliance before the first delivery.
Non-Negotiable Certificate of Analysis Parameters
A CoA that lists only viscosity and appearance is not a compliance document; it is a shipping confirmation. For silicone polymer and siloxane procurement, the CoA must specify:
- Volatile content by weight loss per ISO 3251 (typically 105°C, 3 h for standard PDMS grades), reported as a percentage. Standard grades commonly run <1.0%; extrusion or coating grades with stricter outgassing requirements may need <0.3%.
- Cyclosiloxane assay (D3–D6) by GC-MS headspace — total D3+D4+D5+D6 combined. A working specification limit of <500 ppm total is commonly applied in industrial adhesive and sealant grades; electronics and medical applications often tighten this to <100 ppm or lower. Detection capability at 1–10 ppm by GC-MS headspace is achievable in a properly equipped laboratory.
- Organotin catalyst residual by ICP-OES, reported as Sn in ppm. For non-food, non-medical silicone: <20 ppm is a common industrial threshold; for food-contact and medical grades, <2 ppm is the appropriate target, reflecting FDA 21 CFR and ISO 10993-13 extractables risk management.
- Chloride content, particularly for chlorosilane-derived materials, where residual HCl or chloride ions drive downstream corrosion, cure inhibition, and respiratory hazard in heated application environments. A limit of <50 ppm chloride is a defensible starting point for general grades.
- Heavy metals (Pb, Cd, Hg, Cr VI) per IEC 62321 or equivalent for electrical/electronic applications — mandatory for RoHS compliance and increasingly demanded in food and pharma supply chains.
- Viscosity tolerance stated as a percentage band around nominal (e.g., ±10% for general grades, ±5% for precision dispensing applications), since MW distribution shifts correlate with oligomer content changes that GC-MS may not always catch batch-to-batch before product performance drifts.
Procurement specification reference table:
| Parameter | Test Method | Specification Limit — Standard Grade | Specification Limit — Medical/Food Grade | Regulatory Basis |
|---|---|---|---|---|
| Volatile content | ISO 3251 | ≤1.0% w/w | ≤0.3% w/w | REACH Article 33; FDA 21 CFR 175.105 |
| D4+D5+D6 total | GC-MS headspace | ≤500 ppm | ≤100 ppm | REACH Annex XIV (D4); CEPA Schedule 1 (D4); Prop 65 (D4) |
| Organotin residual (Sn) | ICP-OES | ≤20 ppm | ≤2 ppm | ISO 10993-13; FDA extractables guidance |
| Chloride content | Potentiometric titration / IC | ≤50 ppm | ≤10 ppm | OSHA HCl PEL (5 ppm ceiling) — processing risk basis |
| Heavy metals (RoHS set) | IEC 62321 | Per RoHS limits | Per RoHS + USP | RoHS Directive 2011/65/EU; USP elemental impurities |
| Viscosity (at nominal) | ISO 3219 / ASTM D1084 | Nominal ±10% | Nominal ±5% | Internal product performance; MW distribution proxy |
Operational warning — The viscosity drift trap: A supplier who cannot hold viscosity within specification is also unlikely to hold oligomer content within specification, because both are outputs of the same polymerization control window. Plants that accept loose viscosity tolerances in the name of “it still processes fine” often find D4/D5 batch variance is the cause of intermittent QA rejects months later, with no obvious connection to the CoA they approved.
SDS Quality Audit: Reading the Document as a Compliance Artifact
Before placing a first order, audit the supplier’s SDS against three specific failure points that reveal whether their regulatory knowledge is current:
- Section 2 (Hazard Identification): Does it correctly identify D4 as a REACH Annex XIV SVHC and D5 as PBT-classified? A 2024-vintage SDS that still reads “not classified as hazardous” for a D4-containing material above 0.1% w/w is a red flag — either the regulatory team is outdated or the product formulation is undisclosed.
- Section 8 (Exposure Controls): Does it cite jurisdiction-specific OELs — OSHA PELs, ACGIH TLVs, or the UK BOHS 10 ppm working reference for total siloxane — rather than the legally useless phrase “ensure adequate ventilation”? Generic language here means your EHS team will have no engineering basis for LEV design.
- Section 11 (Toxicological Information): Does it distinguish between the polymer matrix hazard profile and the residual monomer/oligomer hazard? A single toxicity statement covering “silicone” as a category conflates high-MW PDMS (low acute hazard) with reactive cyclosiloxane residuals — a distinction that matters enormously for reproductive toxicity classification under Prop 65 and REACH.
Supplier Audit Questions That Reveal Process Maturity
The questions you ask before award reveal more than any certification. Four questions with genuine diagnostic value:
- “What is your in-process D4/D5 monitoring frequency, and can you share batch-level data going back 24 months?” A supplier managing cyclosiloxane content — not just testing at lot release — will have trend data. Suppliers without it are testing to pass, not managing to specification.
- “What is your catalyst quenching protocol after polymerization, and how do you verify residual tin before packaging?” The answer reveals whether ICP-OES is a routine step or an occasional audit.
- “How do you validate low-oligomer claims across seasonal or feedstock variation?” Chlorosilane monomer quality varies with upstream supply; a robust supplier compensates with adaptive process control, not just end-of-line testing.
- “Can you provide your REACH registration numbers for all [silane monomers](https://siliconchemicals.com/silane-monomers/) feeding this product?” For buyers in medical, pharma, or food packaging — the Tier-2 supply chain matters. A PDMS that is itself compliant can still carry a regulatory liability if the upstream monomer lacks a valid REACH registration, because you inherit the supply chain’s documentation gaps.
Contractual Mechanisms That Give Specifications Teeth
Embedding a specification sheet as a purchase order exhibit — rather than a side document — creates a deviation notification obligation rather than a voluntary disclosure. Contracts should include:
- A right-to-audit provision covering EHS process controls and QA laboratory records, exercisable with reasonable notice (30–60 days is typical in chemical supply agreements).
- A SCAR (Supplier Corrective Action Request) trigger tied specifically to out-of-specification results on cyclosiloxane assay, organotin residual, or volatile content — not just customer complaints. Complaints come after a failure has already reached your line.
- A material change notification clause requiring advance disclosure of any monomer source change, catalyst system change, or manufacturing site change — each of which can shift the toxicity-relevant impurity profile without changing the nominal product specification.
A food-contact clearance under FDA 21 CFR 175.105 means the silicone material poses no extractables risk at any processing temperature.False
FDA 21 CFR 175.105 grants clearance for high-MW PDMS in food-contact applications under defined conditions, but it does not eliminate extractables risk at elevated temperatures. PDMS thermal depolymerization onset begins as low as 150°C with trace catalyst, generating cyclosiloxane oligomers that may migrate into food matrices. Clearance is conditional on the specific polymer grade, MW range, and processing conditions — not a blanket zero-risk declaration.
In a typical high-volume electronics assembly operation running three shifts on a silicone conformal coating line, the coating supplier’s standard CoA reported volatile content at 0.8% — within the generic specification. A downstream customer QA failure triggered an investigation, which found D4+D5 running at 380–420 ppm batch-to-batch, well under no stated limit because the purchase order had never specified one. The fix was straightforward: add the GC-MS cyclosiloxane limit to the specification sheet and require batch-level data at delivery. The underlying process hadn’t changed — only what was being measured and contracted.
Vertically integrated organosilicon manufacturers that operate in-house GC-MS, ICP-OES, and FTIR analytical laboratories — and maintain dedicated QA documentation teams — provide the data infrastructure that makes this level of procurement control practical rather than aspirational. When a supplier can provide batch-level cyclosiloxane trending data, upstream monomer REACH registration numbers, and catalyst residual certificates from the same production chain, your compliance team is working from evidence rather than assumption.
Quick verdict: If a silicone supplier cannot provide batch-level D4/D5 GC-MS data on request and a current SDS with jurisdiction-specific OELs in Section 8, they have not yet invested in the analytical infrastructure your compliance obligations require — treat the gap as a qualification failure, not a paperwork request.














