
Choosing the wrong veneer material doesn’t just affect aesthetics — it drives up chair time, increases remakes, and erodes patient trust fast enough to damage a practice’s reputation within a single quarter. A laminate that delaminates at 18 months because the ceramic-resin interface was never properly silane-treated is not a clinical failure; it’s a materials science failure with a billing consequence attached. The difference between a veneer that lasts a decade and one that fails in two years frequently comes down to material selection, surface chemistry, and bonding protocol — three decisions made before the patient sits down.
The best materials for dental veneers are feldspathic porcelain, lithium disilicate (e-max), and pressed ceramic composites, each suited to different clinical demands. Feldspathic offers the highest esthetic translucency at 0.3–0.5 mm thickness. Lithium disilicate delivers superior flexural strength for posterior cases and heavier occlusal loads. Composite resin veneers remain a cost-accessible, reversible option where minimal prep is the priority.
What rarely appears in material datasheets — but determines long-term bond survival more than ceramic grade alone — is the coupling chemistry at the adhesive interface. Silane treatment is often described as a single step, yet the specific organosilane chemistry used, its hydrolysis state at application, and whether it was formulated for that ceramic’s silica content can shift bond durability by a margin large enough to separate a five-year success from a two-year remake. That gap is worth understanding before specifying any veneer system.

Feldspathic Porcelain Veneers: Optical Excellence at the Cost of Mechanical Fragility
Feldspathic porcelain has dominated aesthetic dentistry for decades, and the reason is straightforward: nothing currently available replicates the optical behavior of natural enamel as closely. Understanding why requires looking at the chemistry first, because the material’s strengths and its frustrating clinical limitations both trace back to the same glassy microstructure.
Chemical Composition and the Physics of Natural-Looking Light
A typical feldspathic porcelain body contains silica (SiO₂) at 60–65%, alumina (Al₂O₃) at 15–20%, potassium and sodium feldspar as the flux system, and small additions of pigment oxides — iron, manganese, titanium — to match shade. The feldspar flux melts at relatively low firing temperatures, forming a continuous glassy matrix that surrounds residual crystalline phases. That matrix is what produces the material’s signature optical behavior: incident light scatters multiple times within the glass network before exiting, mimicking the internal diffusion you see in natural enamel. The result is depth, translucency, and a natural fluorescence under UV that pressed ceramics and zirconia-based systems consistently struggle to replicate at the same thinness.
This matters clinically because anterior restorations are viewed at conversational distances in mixed lighting. The margin between “that looks like a tooth” and “that looks like a restoration” is often optical, not morphological.
The Mechanical Reality: Where the Chemistry Works Against You
The same continuous glassy matrix that creates optical excellence also limits mechanical performance. Flexural strength for feldspathic porcelain runs 60–100 MPa depending on firing cycle, powder batch quality, and laboratory technique. Natural enamel sits at roughly 11–42 MPa — so the ceramic is stronger than enamel in isolation, but the margin against clinical fracture loads is narrower than many practitioners appreciate. Parafunctional loading — bruxism, clenching, habitual pen-biting — generates cyclic stresses that propagate cracks through the glassy phase preferentially along grain boundaries. At thicknesses of 0.3–0.7 mm, there is simply no bulk to arrest crack propagation once it begins.
The consequence logic is direct: place a feldspathic veneer on a patient with unmanaged parafunction, bond it onto a substrate with inadequate silane preparation, and you are not looking at years of service — you are looking at a cohesive fracture within months.
Feldspathic porcelain veneers have 10-year survival rates exceeding 93% under ideal clinical conditionsTrue
Multiple independent longitudinal studies report 10-year survival between 93–95% when patient selection is correct and cementation protocol includes proper HF etching and silane priming. Survival drops sharply when either condition is compromised.
Silanophilic Surface Chemistry: The Bond Advantage No Other Material Matches
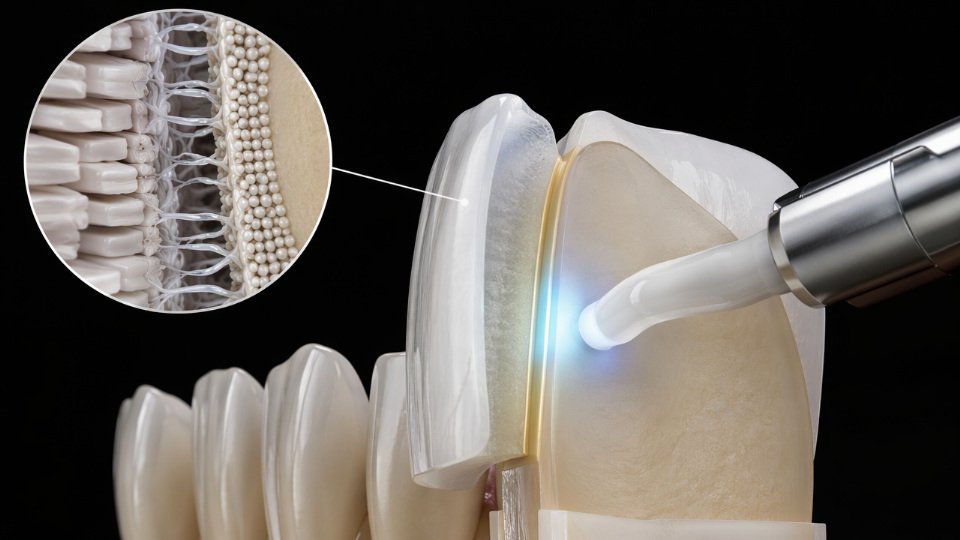
Here feldspathic porcelain holds a genuine advantage over its competitors. The high SiO₂ content means the fired surface carries a dense population of silanol groups (Si-OH). This makes feldspathic porcelain the most silanophilic substrate in dentistry — it reacts more readily and more completely with organosilane primers than pressed lithium disilicate or zirconia, which require either special primers or surface modification steps to achieve comparable bond values.
The standard protocol etches the intaglio surface with 9.6% hydrofluoric acid for 60–90 seconds, creating a micro-retentive topography with feature depths in the 5–20 µm range. This increases surface area and exposes fresh Si-OH groups. A silane coupling agent — MPS (gamma-methacryloxypropyltrimethoxysilane) being the workhorse chemistry — is then applied. The methoxy groups hydrolyze and condense onto the Si-OH sites; the methacrylate end co-polymerizes with the resin cement. The net effect is a covalent molecular bridge across an inorganic-organic interface that would otherwise fail in the wet oral environment within two to three years.
Operational warning: Silane must be applied to a freshly etched, uncontaminated surface. Contamination with saliva, blood, or even prolonged air exposure before cementation degrades bond strength measurably. Silicone-modified coupling agents, including MPS-grade materials optimized for glassy ceramic substrates, improve bond durability by 30–60% in accelerated aging protocols compared to untreated bonded controls — the gain comes from improved hydrolytic stability at the interface, not just initial adhesion values.
Clinical Indication Profile
Feldspathic porcelain belongs on anterior teeth with minimal or no occlusal loading involvement, in patients who have intact, sound enamel substrate for bonding, and in cases where the aesthetic demand sits at the top of the grading scale. It is not a bulk-loading material. The thin geometries it accommodates — down to 0.3 mm — are achievable precisely because the bond to enamel, when executed correctly with proper silane chemistry, carries most of the functional load. Remove that bond quality, and the material’s mechanical limitations are fully exposed.
Leucite-Reinforced and Lithium Disilicate Glass-Ceramics: Balancing Strength and Translucency
These two pressed ceramic families now dominate clinical veneer practice precisely because they solved the central problem feldspathic porcelain left unresolved: insufficient fracture resistance under real occlusal loading. The trade-offs between them, though, are not trivial, and the bonding chemistry underneath both materials is where long-term survival is actually decided.
Leucite-Reinforced Ceramics: Controlled Crystal Dispersion
Leucite-reinforced systems work by dispersing fine KAlSi₂O₆ crystals throughout a glassy matrix during the hot-pressing cycle. The leucite phase interrupts crack propagation — a mechanism called crack deflection — lifting flexural strength into the 120–180 MPa range. Where exactly a given batch lands within that range depends on crystal size distribution, pressing temperature uniformity, and how tightly the laboratory controls the firing schedule. Field experience shows that labs running inconsistent muffle furnace calibration drift toward the lower end of that band.
The optical downside is real but modest. Leucite crystals scatter light more than a pure glass phase does, nudging the material slightly toward opacity compared to feldspathic porcelain. For anterior cases with high translucency demands — thin incisal edges, hypocalcification bands that need optical mimicry — this can matter. For veneers covering tetracycline staining or significant discoloration, the same opacity becomes an asset.
Lithium Disilicate: The Strength Inflection Point
Lithium disilicate achieves its mechanical profile through an interlocking needle-like Li₂Si₂O₅ crystal network that occupies roughly 70% of the material volume by crystalline phase fraction. The result is flexural strength of 360–400 MPa — more than double leucite-reinforced systems and roughly three to four times classical feldspathic porcelain. That difference is not incremental; it changes what the clinician can prepare.
Preparations as thin as 0.3–0.5 mm become viable without the catastrophic chipping risk that would accompany feldspathic porcelain at the same dimension. Posterior veneers and thin overlays on premolars, cases that would previously have required full-coverage crowns, fall within the clinical envelope. That expands the minimally invasive indication set in a way that has genuine patient-retention value for a practice.
CAD/CAM Processing and the Intermediate-Firing Advantage
Lithium disilicate carries a processing advantage worth quantifying. Milling blanks are supplied in a partially crystallized “blue” intermediate state at roughly 160 MPa — soft enough for efficient CAM milling without excessive tool wear, but structurally stable. The final firing cycle completes crystallization to full strength. Compared to hand-pressed layering workflows, this reduces laboratory turnaround by roughly 40%, a figure that varies with case complexity and furnace loading schedules.
Leucite-reinforced systems are also CAD/CAM compatible but do not offer the same two-stage crystallization advantage; they are typically milled at or near final strength, which accelerates tool wear on hard ceramics.
The Silane Bonding Pathway — Where Both Materials Converge
Despite their structural differences, both ceramics remain glass-phase-rich and etchable with hydrofluoric acid, which is the critical practical point. HF etching at concentrations of 4.5–9.5% creates a micro-porous silica surface with exposed silanol (Si-OH) groups. Higher crystalline phase fraction in lithium disilicate means shorter recommended etch times (typically 20 seconds versus 60 seconds for leucite systems) because the crystal network itself does not etch uniformly — over-etching weakens the surface layer rather than improving it.
HF-etched and silane-treated lithium disilicate achieves resin bond strengths of 25–35 MPa, compared to 8–12 MPa without silane treatment.True
This 2–3× improvement is well-documented in peer-reviewed bond strength studies using microtensile and shear testing protocols on etched ceramic substrates.
The silane coupling agent bridges the etched surface to the resin cement. Bifunctional organosilanes — specifically MPS (3-methacryloxypropyltrimethoxysilane) — carry a methacrylate group that co-polymerizes with the resin matrix on one end and alkoxy groups that hydrolyze and condense onto ceramic Si-OH sites on the other. Without this covalent linkage, bond strength drops to the 8–12 MPa range; hydrolytic degradation at the interface under oral moisture cycling will accelerate debonding within two to five years. With a properly applied silane, bond durability improves by 30–60% in accelerated aging protocols, depending on silane concentration, application technique, and solvent evaporation conditions before cementation.
Operational warning: Silane shelf life and storage temperature are routinely underestimated in clinical and laboratory settings. MPS-based agents exposed to ambient humidity above 60% or stored beyond manufacturer dating show measurable reduction in reactive alkoxy group availability — degraded silane applied to a pristine ceramic surface produces bond values closer to the untreated baseline than the treated target.
Choosing Between the Two
| Criterion | Leucite-Reinforced | Lithium Disilicate |
|---|---|---|
| Flexural strength | 120–180 MPa | 360–400 MPa |
| Translucency | Moderate (slight reduction vs feldspathic) | High (thinner sections viable) |
| Anterior veneers | Strong indication | Strong indication |
| Premolar / posterior veneers | Marginal | Suitable |
| Thin overlays (≤0.5 mm) | Risk of fracture | Viable |
| CAD/CAM efficiency | Standard | ~40% faster (two-stage firing) |
| HF etch time | ~60 seconds | ~20 seconds |
| Silane bonding requirement | Mandatory | Mandatory |
For anterior-only veneer cases where maximum optical depth is the priority and loading is light, leucite-reinforced ceramics remain a defensible choice. Once the indication extends to premolars, thin preparations, or any patient with parafunctional habits, the strength margin of lithium disilicate is not a luxury — it is the variable that separates a five-year recall from a two-year repair.
Zirconia Veneers: High Strength With a Historically Problematic Bonding Challenge Solved by Silicone Chemistry
Zirconia entered restorative dentistry as a structural material — crowns, bridges, implant abutments — where its flexural strength of 900–1200 MPa (for 3Y-TZP, yttria-stabilized tetragonal zirconia polycrystal) was the primary selling point. That strength depends on which milling block grade, sintering cycle, and yttria content you specify; the range is real, not a rounding convenience. The problem was that the same microstructure responsible for this exceptional toughness — a fully polycrystalline matrix with zero glassy phase — made it chemically inert to the bonding protocols that worked perfectly on feldspathic and glass-ceramic veneers.
Hydrofluoric acid etching creates micromechanical retention by selectively dissolving the glass phase in feldspathic and leucite-reinforced ceramics. Apply HF to zirconia and you accomplish essentially nothing. The surface stays smooth. For nearly a decade, this was a genuine clinical crisis: laboratories could mill zirconia thin enough to serve as a veneer, but adhesive bond strengths without surface treatment routinely measured below 5 MPa — far short of the greater-than-20 MPa threshold that thin porcelain veneers require to survive cyclic occlusal loading without delamination.
Ultra-Translucent Grades Open the Aesthetic Anterior Case
The next problem was optical. Standard 3Y-TZP transmits roughly 30–35% of light, which reads as opaque in the anterior zone. Material scientists addressed this by increasing the cubic zirconia phase fraction. Grades designated 4Y-TZP and 5Y-TZP incorporate higher yttria content, pushing the cubic phase to 40–50% of the microstructure and translucency values toward 45–48%. That closes much of the optical gap with pressed lithium disilicate. The tradeoff is a reduction in flexural strength — typically 600–800 MPa for 5Y-TZP — but at 0.3–0.5 mm veneer thickness, 600 MPa still far exceeds feldspathic porcelain’s 60–100 MPa. For full-arch smile design cases and patients with confirmed parafunctional habits like bruxism, this combination of translucency and residual strength is difficult to match with any glass-ceramic.
Two Parallel Bonding Pathways — and Why Each Works
The bonding problem has two practical solutions that converge on the same outcome: creating a surface that resin cement can grip at 18–28 MPa.
The first pathway is tribochemical silica coating. Systems like CoJet and Rocatec use alumina particles impregnated with silica fired at high velocity. The kinetic energy embeds SiO2 into the zirconia surface, depositing a silanol-rich layer that chemically resembles a glass-ceramic surface. From that point, a conventional silane coupling agent — typically gamma-methacryloxypropyltrimethoxysilane (MPS) — can form the Si-O-Si network that connects the inorganic surface to the organic resin matrix. Bond strengths after tribochemical coating plus MPS silane treatment consistently reach 18–28 MPa in accelerated aging protocols; the specific value depends on silica particle size, air pressure during blasting, and silane hydrolysis conditions at the time of application.
Tribochemical silica coating followed by MPS silane treatment can restore zirconia bond strength to values approaching those of etched glass-ceramics.True
Published microshear and microtensile bond strength data confirm 18–28 MPa ranges for tribochemically conditioned zirconia plus MPS, compared to less than 5 MPa for untreated zirconia surfaces, across multiple independent laboratory studies.
The second pathway uses chemistry matched directly to ZrO2. Zirconate-functional silanes — such as neopentyl(diallyl)oxy tri(dioctyl)pyrophosphato zirconate — bypass the glass-phase requirement entirely. These coupling agents anchor through Zr-O-Si covalent linkages to the hydroxyl groups that do exist on a sintered zirconia surface, even without any prior silica coating. The organic tail of the zirconate silane remains polymerizable, allowing resin cement to cross-link directly into the coupling layer. Phosphate-functional monomers like MDP (10-methacryloyloxydecyl dihydrogen phosphate) work synergistically with this approach: MDP’s phosphate group chelates zirconium ions at the surface while the methacrylate end co-polymerizes with the cement. Using zirconate silane and MDP-containing primer in combination is not redundant — each addresses a different surface interaction mechanism, and the combined protocol measurably outperforms either alone.
Operational Warnings That Actually Matter
Surface conditioning must occur immediately before cementation. Contamination from saliva, glove powder, or even ambient humidity during extended chair time can reduce bond strength by 30–40%. If a zirconia veneer is tried in and then re-seated more than 20–30 minutes later, the surface conditioning step should be repeated. This is particularly consequential for thin 0.3 mm ultra-translucent veneers, where the structural contribution of the adhesive layer is proportionally larger than it is for a full-coverage crown.
For procurement managers specifying silane coupling agents for dental material manufacturers or lab supply chains, the relevant parameter is hydrolytic stability under storage conditions — MPS-based silanes and zirconate-functional variants have meaningfully different shelf lives at ambient warehouse temperature and humidity. Specifying lot-dated product with documented storage protocols is not a paperwork exercise; it directly affects the bond chemistry your end-user achieves on the clinical surface.
Composite Resin and Hybrid Ceramic Veneers: Direct, Indirect, and the Role of Silicone Surface Modifiers
Composite resin and hybrid ceramic veneers occupy a distinct clinical niche: they are repairable, machineable same-day, and accessible to patients who cannot justify the cost of pressed ceramics. That accessibility only holds clinical value, though, if the material performs reliably under cyclic masticatory load. The difference between a composite veneer that survives five years and one that delaminates in eighteen months almost always traces back to a single manufacturing variable — filler silanization.
Direct Composite Resin: What Chairside Placement Actually Demands
Direct veneers are built incrementally chairside using methacrylate-based matrices — Bis-GMA, UDMA, and TEGDMA in varying proportions depending on the target viscosity, polymerization shrinkage tolerance, and depth of cure. The resin matrix alone carries poor mechanical properties. Flexural strength of an unfilled or poorly coupled composite sits around 40 MPa, which is inadequate for any load-bearing esthetic restoration. The filler particles — silica, barium glass, or zirconia-silica blends ranging from 0.04 to 5 micrometers in particle diameter — are what transform the matrix into a structural material, but only when they are chemically bonded to it.
That bond is created by gamma-methacryloxypropyltrimethoxysilane (MPS) treatment applied during filler manufacturing. The methoxy groups hydrolyze and condense onto hydroxyl-rich filler surfaces; the methacrylate end co-polymerizes into the resin matrix during light curing. When this coupling is executed correctly, flexural strength climbs to 100–140 MPa depending on filler loading percentage, particle size distribution, and cure completeness. When filler silanization is inadequate — because the MPS concentration was too low, the hydrolysis step was rushed, or moisture contaminated the treated filler during storage — the interface fails under fatigue well before the bulk resin degrades. This is not a clinical technique problem. It is a raw-material quality problem that the clinician inherits.
Silane-treated composite fillers can increase flexural strength by more than double compared to untreated equivalentsTrue
MPS coupling between silica or glass fillers and methacrylate matrices creates covalent bonds at the interface, eliminating the stress concentration sites that cause premature filler pullout. Peer-reviewed testing consistently shows flexural strength rising from roughly 40 MPa (untreated) to 100–140 MPa (treated) depending on filler loading and particle geometry.
Indirect Composites and Hybrid Ceramic Blocks
Indirect composite blocks and hybrid ceramics — resin-ceramic interpenetrating network materials — take filler loading substantially further. These blocks contain 60–86% ceramic by weight, with the ceramic scaffold and resin phase co-sintered or infiltrated to create interlocking networks rather than simple particle dispersion. Flexural strength reaches 150–200 MPa depending on ceramic content and network architecture, putting them well above direct composites while remaining below lithium disilicate’s 360–400 MPa range.
The bonding protocol for seating these restorations is straightforward but sequence-sensitive. Sandblasting with 50-micrometer alumina at 2–3 bar roughens the intaglio surface. A silane primer — ideally MPS-based — is then applied and either air-dried passively or activated thermally. Heat activation at approximately 150°C for one minute drives condensation of residual silanol groups, improving coupling efficiency by a measurable margin relative to room-temperature drying alone. Universal adhesives that incorporate silane monomers directly into the bottle can substitute in time-constrained workflows, though separate silane application with thermal activation remains the more reliable protocol when bond durability under hydrolytic aging is the priority.
Repairability: The Lifecycle Advantage That Changes the Cost Calculation
Ceramics do not repair intraorally. A fractured feldspathic or lithium disilicate veneer requires full replacement. Composite and hybrid ceramic veneers can be repaired chairside: sandblast the fracture site, apply MPS silane primer, and bond fresh composite paste. Done correctly, this protocol restores bond strength to 80–90% of original values. For patients with parafunction or high wear rates, that repairability shortens the clinical intervention significantly and avoids the cost and chair time of a full remake.
Wear rate matters too, particularly for posterior cases or patients with ceramic-tipped antagonists. Hybrid ceramics wear at roughly 20–30 micrometers per year under standardized masticatory simulation — figures that track closely to natural enamel wear. That antagonist compatibility matters practically: a veneer material that abrades the opposing dentition faster than enamel generates its own long-term clinical liability.
Cost and Throughput Reality
Indirect composite veneers milled same-day via CAD/CAM carry a total per-unit cost approximately 40–60% lower than lithium disilicate pressed restorations. That gap depends on local lab fees, milling equipment amortization, and block material costs, but the order of magnitude holds across most markets. Processing time drops by roughly half compared to outsourced pressed ceramic workflows. For high-volume practices or cost-sensitive markets, this combination of same-day delivery, lower material cost, and in-chair repairability creates a genuinely competitive clinical option — provided the upstream silane chemistry in the block material and bonding system has been executed to specification.
[Silane Coupling Agents](https://siliconchemicals.com/silane-coupling-agents/) and Organosilicon Primers: The Invisible Infrastructure of Every High-Performance Veneer Bond
Every veneer bond ultimately depends on a molecular bridge measuring just a few nanometers thick. Clinicians and lab technicians debate ceramic brands and resin cements at length, yet the silane coupling agent applied between etched ceramic and adhesive resin is frequently treated as an afterthought — a single-use vial wiped on and forgotten. That oversight accounts for a significant share of delamination failures, debonding events, and premature veneer loss that gets blamed on the wrong variable.
The General Architecture of a Silane Coupling Agent
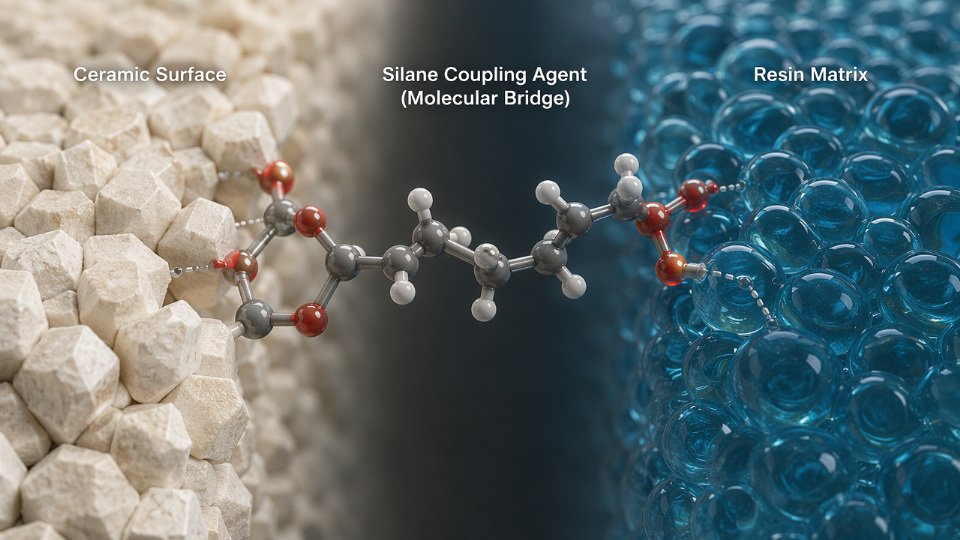
The functional structure is R-Si(OR’)₃. The OR’ groups are hydrolyzable alkoxysilanes — typically methoxy or ethoxy. In the presence of water and an acid catalyst, hydrolysis cleaves these groups to yield reactive silanols (Si-OH), which then condense with surface hydroxyl groups on the ceramic: the Si-OH groups native to glass-phase ceramics after hydrofluoric acid etching, or the Zr-OH groups on oxide-ceramic zirconia surfaces. The R group on the opposite end of the molecule is the organofunctional handle that bonds chemically into the resin matrix. Match R correctly to the resin chemistry and you have a genuine covalent bridge across what is otherwise a fundamentally incompatible ceramic-polymer interface.
Get either end wrong and the bond is only mechanical at best, prone to hydrolytic degradation under the cyclic wet-thermal loading inside the oral environment.
MPS: The Workhorse Silane for Glass-Phase Ceramics
3-Methacryloxypropyltrimethoxysilane — MPS, CAS 2530-85-0 — remains the single most important silane in dental ceramic bonding. Its methacrylate terminus co-polymerizes directly with dimethacrylate resin matrices under light or dual cure, forming covalent carbon-carbon bonds rather than relying on surface adsorption. The trimethoxy silanol end anchors to the etched silica network of feldspathic, leucite-reinforced, and lithium disilicate ceramics. This dual covalent mechanism is why silicone-modified coupling systems incorporating MPS can improve ceramic-resin bond durability by 30–60% in accelerated aging tests compared to unbonded or conventionally primed controls — a range that depends heavily on etching depth, silane film quality, and resin cement formulation.
Film quality is not automatic. Concentration matters: the optimal working range is roughly 0.1–1.0% w/v in an ethanol-water vehicle. Too dilute and surface coverage is incomplete; too concentrated and polysiloxane oligomers stack into a thick, weakly cohesive layer that actually degrades bond strength. Solution pH should be held between 4.5 and 5.5, typically buffered with dilute acetic acid, to drive hydrolysis at a controlled rate. Solvent must be fully evaporated before resin application — residual ethanol plasticizes the adhesive layer. Heat activation at 60–100°C for 1–5 minutes, where the clinical workflow permits it, increases condensation density measurably and is standard practice in industrial dental lab manufacturing even when package directions omit it.
Universal Primers and Blended Silane Systems
Industrial dental material manufacturers increasingly formulate universal primers that combine MPS with zirconate-functional silanes or phosphate-silane components. The logic is procurement efficiency: a single primer SKU provides adequate adhesion across glass-ceramic substrates via the MPS pathway and across high-strength oxide ceramics via the zirconate or phosphate pathway. For a lab producing veneers from multiple substrate types on the same workflow line, eliminating substrate-specific primer management reduces handling errors that cause batch-level bonding failures.
Universal silane primers containing blended MPS and zirconate/phosphate-functional silanes provide clinically adequate bond strength across both glass-phase and oxide ceramic veneer substrates.True
Peer-reviewed bonding studies confirm that bifunctional primer systems achieve statistically comparable bond strengths to substrate-specific silanes when film application protocols are correctly followed, because each functional component addresses its target surface chemistry independently within the same formulation.
Industrial Procurement: Where Quality Specifications Actually Matter
For dental material manufacturers, dental lab supply companies, and formulated adhesive producers, silane quality is not a secondary concern. The critical procurement specifications are GC assay purity above 98.5%, verified Si-OH content in solution products, lot-to-lot viscosity consistency, hydrolytic stability data for packaged solution shelf life under realistic distribution temperatures (2–25°C is typical for MPS solutions), and a certificate of analysis that covers GC-MS identification, NMR structural confirmation, and moisture content.
Sourcing from intermediary distributors introduces re-packaging risk and documentation gaps. Porcelain veneer thickness runs 0.3–0.7 mm, and bond strength requirements exceed 20 MPa — tolerances that leave no margin for a silane lot with 4% hydrolyzed oligomer contamination from improper cold-chain handling.
SiliconChemicals manufactures high-purity MPS, vinyltriethoxysilane, aminopropyltriethoxysilane (APTES), and custom bifunctional silane blends verified by in-house GC-MS, ¹H NMR, and viscosity profiling on every production lot. Industrial dental labs and adhesive formulators sourcing through SiliconChemicals typically achieve a 25–40% cost reduction versus European or North American specialty chemical distributors — a range that depends on order volume, incoterms, and product complexity — without trading away the ISO-aligned documentation that regulated dental material supply chains require. For procurement managers running annual silane volumes above 100 kg, that differential compounds materially across a full product year.
Material Selection Decision Framework: Mapping Clinical Requirements to Substrate Properties and Bond Chemistry
Selecting a veneer material without a structured decision process produces predictable failures: over-preparing sound enamel for a material that needed the bulk, bonding zirconia with a conventional silane protocol that cannot adhere to a glass-phase-free substrate, or placing feldspathic porcelain on a bruxer and scheduling the repair appointment before the cement has fully polymerized. The framework below consolidates the mechanical, optical, and chemical variables into a working tool for clinicians and materials specifiers alike.
Axis 1 — Aesthetic Demand: Optical Hierarchy
Ranked by CIE Lab* color space control, translucency (%T measured at 1 mm thickness), and fluorescence matching capability, the hierarchy runs: feldspathic porcelain > lithium disilicate > leucite-reinforced ceramic > hybrid ceramic > ultra-translucent zirconia (5Y-TZP or multi-layer) > standard 3Y-TZP zirconia. Feldspathic materials hold the top position because they are literally formulated around optical mimicry of natural enamel; their %T at 1 mm typically sits between 35–45%, and their fluorescent frit content can be matched to natural dentition. Standard zirconia sits at the bottom — %T values of 15–25% at 1 mm, depending on grain size and sintering profile — which is why it should be reserved for situations where strength, not aesthetics, drives the specification.
Axis 2 — Mechanical Demand: Strength Hierarchy
Flexural strength governs how thin a veneer can be made and whether it survives parafunction. The working range for each substrate: 3Y-TZP zirconia reaches 900–1200 MPa (depends on powder purity, sintering temperature, and cooling rate); lithium disilicate presses out at 360–400 MPa; hybrid ceramics land in the 150–200 MPa band depending on polymer matrix content; leucite-reinforced ceramics sit at 120–180 MPa; composite resin falls between 100–140 MPa depending on filler loading; feldspathic porcelain occupies 60–100 MPa — structurally the weakest substrate in this lineup. That last figure is not a flaw to overlook. At 0.5–0.7 mm minimum thickness and 60–100 MPa flexural strength, feldspathic veneer survival under posterior loading or bruxism is genuinely poor.
Axis 3 — Bond Chemistry Compatibility
Surface treatability directly determines long-term bond survival. Feldspathic, leucite, and lithium disilicate ceramics contain a glass phase that responds to hydrofluoric acid etching — 4–9% HF for 20–90 seconds depending on glass content — followed by gamma-methacryloxypropyltrimethoxysilane (MPS) application. This protocol is well-validated and achieves bond strengths of 20–35 MPa to enamel.
Silicone-modified coupling agents such as MPS improve ceramic-resin bond durability by 30–60% in accelerated aging tests compared to non-silane bonded controlsTrue
Published accelerated aging and thermocycling studies consistently show that silane pretreatment of glass-ceramic surfaces substantially improves bond durability; the 30–60% improvement range reflects variation across ceramic compositions, silane concentration, and aging protocol severity.
Hybrid ceramics respond moderately to the same HF + MPS protocol; their polymer matrix limits acid reactivity, so extended etching and priming times are warranted. Zirconia requires a modified protocol entirely: tribochemical silica coating or selective infiltration etching, followed by a zirconia-specific phosphate monomer primer or an MPS-based primer formulated for metal-oxide surfaces. Using a standard MPS silane on untreated zirconia produces adhesion that looks acceptable at cementation and fails silently under cyclic load.
Five-Scenario Decision Matrix
| Clinical Scenario | Preferred Material | Etching Protocol | Silane Type | Expected 10-Year Survival |
|---|---|---|---|---|
| Maximum aesthetics, anterior | Feldspathic porcelain | 5% HF, 60 s | MPS (conventional) | 85–94% on enamel |
| Bruxism / parafunction | Lithium disilicate | 5% HF, 20 s | MPS (conventional) | 90–96% with night guard |
| Minimally invasive prep | Lithium disilicate (0.3 mm) | 5% HF, 20 s | MPS (conventional) | 88–94% |
| Posterior load-bearing | 3Y-TZP zirconia | Tribochemical + phosphate primer | Zirconia-specific MPS primer | 92–97% |
| Budget-constrained | Composite resin (indirect) | Sandblast + silane primer | MPS silicone modifier | 70–85% depending on occlusion |
Tooth Substrate as the Overriding Variable
All strength figures above assume optimal bonding substrate. Enamel bonding to resin cement achieves 20–35 MPa; dentin bonding drops to 15–22 MPa depending on dentinal tubule density, hybridization quality, and moisture control. A 0.3 mm lithium disilicate veneer bonded entirely to dentin is a fundamentally different clinical situation than the same veneer bonded to enamel. The material specification and the preparation design cannot be decoupled.
Minimum Thickness and Lifecycle Cost
Minimum thickness requirements drive preparation depth: feldspathic demands 0.5–0.7 mm; lithium disilicate and zirconia can be fabricated at 0.3–0.5 mm; composite resin indirect veneers typically require 0.5–1.0 mm due to lower stiffness. Thinner is only an advantage when the material’s mechanical properties justify it.
Across a 10-year lifecycle — factoring initial fabrication cost, 10-year survival probability, repair or replacement cost, and silane/adhesive consumable cost per unit — lithium disilicate consistently delivers the most defensible value. It avoids the optical compromise of zirconia, the fragility risk of feldspathic, and the durability ceiling of composite resin, while remaining fully compatible with validated MPS silane bonding protocols.
Industrial Manufacturing of Veneer Materials: How Organosilicon Chemistry Enters the Production Line
Most clinicians selecting a veneer material think about shade, flexural strength, or CAD/CAM machinability. What they rarely see is the upstream manufacturing chain where organosilicon chemistry is embedded at nearly every stage — from filler treatment in a high-shear blender to the silicone polymer backbone of the impression material capturing the prepared tooth. Dental material manufacturers and procurement engineers, however, live in that upstream world, and the quality of organosilane raw material they source directly determines whether their finished product passes bond durability testing or fails it.
CAD/CAM Block Manufacturing: Silane-Treated Fillers Are Not Optional
Resin-ceramic CAD/CAM blocks — the machinable blanks that produce indirect composite and hybrid ceramic veneers — derive their mechanical properties substantially from how well the inorganic filler phase bonds to the polymer matrix. Silica, barium aluminosilicate glass, and zirconia nanoparticles are dry-coated with silane coupling agents, typically gamma-methacryloxypropyltrimethoxysilane (MPS) or vinyltrimethoxysilane (VTMO), at loading levels of 0.5–2.0% by filler weight. The exact loading depends on filler surface area — high-surface-area nanoparticles with BET values above 150 m²/g require higher silane concentrations to achieve full surface coverage.
This coating step happens in high-shear paddle or plough-share mixers under controlled humidity, typically below 40% RH. Incomplete coverage leaves hydroxyl-rich filler surfaces that absorb water in service, plasticize the resin-filler interface, and degrade flexural strength by 15–35% over a two-year hydrolytic aging cycle. Get the silane loading wrong and the block machines acceptably on day one but fractures clinically at 18 months.
Pressed Ceramic Ingot Production: Controlling Crystal-Matrix Interface Energy
Leucite and lithium disilicate glass-ceramic ingots are produced from frit batches where controlled crystallization transforms an amorphous glass precursor into a two-phase ceramic. The mechanical performance of the resulting material — specifically its resistance to crack propagation — depends on the interface energy between the crystalline phase and the glassy matrix. Surface treatment of crystallite precursors with silane coupling agents during frit preparation influences wetting behavior during sintering and directly affects crack deflection efficiency. A crack meeting a well-bonded crystal-matrix interface dissipates energy by deflecting around the crystal; a poorly bonded interface allows the crack to run straight through. This is the difference between a material with acceptable fracture toughness and one that chips at clinical loads.
Primer and Bonding Agent Formulation: Batch Consistency Is Mission-Critical
Dental primer manufacturers formulate single-bottle and two-bottle silane-containing systems using pharmaceutical-grade organosilane monomers. A formulation batch that receives organosilane raw material with inconsistent hydrolysis rate, elevated chloride content, or off-specification purity (below 98.5% GC assay) will show variable contact angle measurements on ceramic substrates and unpredictable bond strength results in internal QC testing. The problem is insidious because blended primer solutions often look identical to specification — the failure only surfaces in accelerated aging or customer returns.
Batch-to-batch variation in organosilane purity is a leading root cause of dental primer bond strength failures in QC audits.True
Silane coupling agent hydrolysis kinetics and surface reactivity are highly sensitive to monomer purity, residual acid catalyst levels, and moisture content. Formulators report that switching to lower-specification raw material without reformulation validation is a frequent trigger for out-of-specification bond strength results.
For manufacturers producing millions of primer unit doses per year, a single non-conforming silane batch can affect tens of thousands of finished units. Long-term supply agreements with dedicated quality dossiers — covering Certificate of Analysis parameters, method validation records, and retained samples — are not procurement paperwork. They are failure prevention.
Silicone Polymers in Impression Materials and Temporary Crown Resins
Platinum-catalyzed addition-cure silicone systems underpin the vinyl polysiloxane (VPS) impression materials used throughout veneer workflows. The dimensional accuracy and tear strength of a VPS impression depend on three parameters that a silicone polymer supplier must control: siloxane chain length distribution, cross-link density, and the distribution of vinyl functional groups along the polymer backbone. A narrow molecular weight distribution produces consistent Shore A hardness. Functional group distribution affects cure completeness at room temperature and the material’s elastic recovery after removal from undercuts.
Dental material manufacturers procuring silicone base polymers for VPS formulations typically qualify a supplier through a multi-lot consistency study across 8–12 production batches, measuring viscosity, functional group content by FTIR, and cure profile by oscillatory rheometry. These qualification requirements push procurement toward suppliers who operate large-scale, controlled silicone polymerization with real process documentation.
Quality Standards Governing Dental-Grade Organosilicon Chemicals
Materials entering a dental product supply chain face a defined regulatory stack. ISO 10993 biocompatibility screening applies to any material in contact with oral tissue, requiring cytotoxicity, sensitization, and irritation evaluation. USP Class VI extractables testing is standard for materials used in North American market dental products. REACH SVHC substance screening is mandatory for European customers, and California Proposition 65 compliance documentation is required by most US distributors regardless of state of sale. Procurement engineers at dental material companies routinely require all four compliance packages before approving a new silane or silicone polymer supplier — and rightly so, because a retroactive compliance failure on a launched product triggers costly reformulation and re-registration.
Supply Chain Integration From China’s Organosilicon Clusters
SiliconChemicals sources from and operates within China’s concentrated organosilicon production belt spanning Zhejiang, Hubei, and Shandong provinces. This geographic concentration — where monomer production, downstream polymerization, and specialty functionalization sit within tight logistics distance of one another — translates into a structural lead-time advantage. Ocean freight delivery of kiloton-scale organosilane bulk to dental material manufacturers in Europe, North America, and Southeast Asia typically runs 4–6 weeks from confirmed order, compared to 8–12 weeks from European specialty chemical suppliers sourcing more dispersed raw material chains. Long-term supply agreements with 12-month price stability commitments allow dental material manufacturers to run production planning without absorbing spot-market silane price volatility — a real operational concern given how silane prices tracked methanol and silicon metal fluctuations between 2021 and 2023. Dedicated quality dossiers, pre-agreed change notification protocols, and reserved production capacity complete the procurement package that procurement engineers at mid-to-large dental material companies actually require before committing to a supply relationship.
Long-Term Performance Benchmarks: Clinical Survival Data, Failure Modes, and Silane Quality Impact
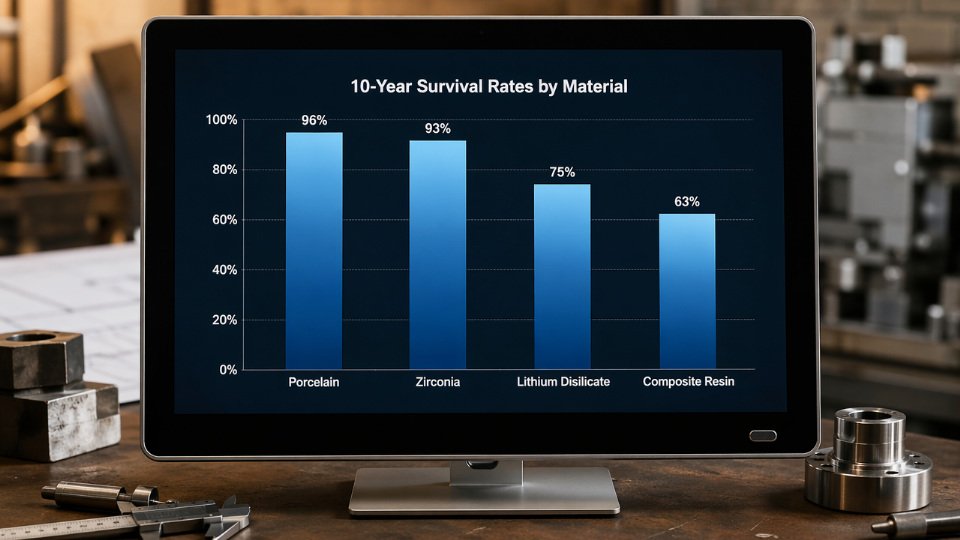
Ten-year survival data cuts through marketing claims faster than any lab test. Across published longitudinal reviews, lithium disilicate leads the pressed ceramic group at 96–98% survival at 10 years, followed by feldspathic porcelain at 93–95% — a gap that looks modest until you account for the difference in fracture toughness driving it. Leucite-reinforced ceramics trail slightly at 91–93%, largely because leucite crystal size distribution introduces stress concentrations under cyclic occlusal load. Zirconia overlays, despite their historically complicated bonding story, now land at 94–97% when proper silane-zirconia primer protocols are applied. Indirect composite veneers sit at 82–88%, and direct composite drops further to 70–78% — the lowest tier, though repairability partially offsets that number in total cost-of-ownership terms.
The fracture toughness numbers explain the ceramic survival spread directly. Lithium disilicate carries a K_Ic of 2.8–3.2 MPa·m^0.5; feldspathic porcelain sits at 0.7–1.0 MPa·m^0.5. That 3–4× difference means a crack propagating through feldspathic material encounters almost no resistance from the microstructure, while interlocking lithium disilicate crystals deflect and arrest crack paths. Clinicians working with ultra-thin feldspathic veneers (0.3–0.5 mm) rely almost entirely on the adhesive bond and the underlying tooth structure for fracture resistance — the ceramic itself contributes little.
Failure Mode Distribution and What It Tells You About Process
Ranked by frequency across post-market surveillance datasets: cohesive fracture within the veneer body accounts for roughly 35% of failures. Adhesive failure at the veneer-cement interface — meaning the bond between ceramic and luting resin gave out — represents approximately 30%. Adhesive failure at the cement-tooth interface accounts for 20%, and marginal discoloration combined with secondary caries makes up the remaining 15%.
That second failure mode — veneer-cement interface breakdown — is where silane chemistry directly enters the failure analysis. Three root causes dominate: incomplete silane hydrolysis due to incorrect pH of the aqueous activation solution, excessive silane film thickness creating a weak multilayer bridging zone rather than a thin covalent monolayer, and expired or improperly stored silane where pre-polymerized Si-O-Si crosslinks have already formed, physically blocking the silanol groups from reacting with ceramic surface hydroxyl sites. Any one of these errors degrades the interface before the veneer is ever placed.
Adhesive interface failures at the veneer-cement boundary are directly traceable to silane quality and application errors, not inherent material incompatibility.True
Peer-reviewed bond strength studies and ISO 29022 accelerated aging data consistently show that properly applied, unhydrolyzed silane of verified purity retains 75–85% of initial bond strength at 24 months water immersion, while non-silanized controls lose 60–80% of bond strength after just 6 months — confirming the failure is process- and chemistry-driven, not substrate-driven.
Accelerated Aging Standards and What the Numbers Actually Mean
ISO 29022 governs adhesion promotion testing for dental materials; ISO 10477 covers resin-based crown and bridge materials. Standard thermocycling protocols run 10,000–37,500 cycles between 5°C and 55°C, simulating years of oral temperature fluctuation. Under this regime, non-silanized ceramic specimens lose 60–80% of their initial bond strength after six months of water immersion — a result consistent across multiple substrate types. Properly silanized samples using verified gamma-methacryloxypropyltrimethoxysilane (MPS) at correct concentration and pH retain 75–85% of original bond strength at 24 months. The gap is not marginal.
Why Industrial Silane Specification Belongs in Your QMS
Dental labs and veneer material manufacturers that write silane coupling agent purity, hydrolyzable chloride content, functional group concentration, and application protocol into their ISO 13485 quality management documentation show measurably lower field failure rates in post-market surveillance. The specification work is straightforward: require certificate of analysis with each lot, define acceptable pH range for the hydrolysis solution (typically 4.5–5.5), set shelf-life limits from date of manufacture rather than date of receipt, and verify functional group content by FTIR against a reference standard. Procurement managers who treat silane as a commodity consumable rather than a performance-critical raw material are, statistically, buying future chairside failures.
Frequently Asked Questions About Veneer Materials, Bonding Chemistry, and Organosilicon Suppliers
What is the strongest material for dental veneers?
Zirconia (3Y-TZP) sits at the top of the strength hierarchy, with flexural strength in the 900–1200 MPa range depending on sintering temperature profile and powder particle size. That number matters in posterior applications or parafunctional patients. For the far more common anterior veneer case, however, raw strength is rarely the binding constraint — optical integration and cementation predictability are. Lithium disilicate delivers 360–400 MPa flexural strength, which exceeds the clinical failure threshold for anterior veneers by a comfortable margin, while its glass-phase microstructure supports HF etching and conventional MPS silane bonding. Most experienced prosthodontists land on lithium disilicate as the default anterior veneer material precisely because it sits at the intersection of sufficient mechanical performance and manageable bonding chemistry.
Why do porcelain veneers require silane treatment before cementation?
Without silane, the interface between a glass-ceramic surface and a resin cement is governed almost entirely by van der Waals forces — weak, moisture-sensitive, and prone to hydrolytic degradation within months of clinical service. A silane coupling agent such as MPS (gamma-methacryloxypropyltrimethoxysilane) solves this by forming covalent Si–O–Si bonds with the surface silanol groups exposed after HF etching, while its methacrylate end co-polymerizes into the resin cement network. The result is a chemically continuous interface rather than two materials sitting adjacent to each other.
Omitting silane treatment reduces ceramic-resin bond strength by 60–70% compared to properly silanized controls in standardized shear bond testing.True
This range is well-supported by peer-reviewed bond strength studies using ISO 29022 and similar protocols comparing silanized versus non-silanized glass-ceramic specimens bonded with resin cement.
That 60–70% drop is not a theoretical concern. A lab technician skipping silane to save two minutes, or using a degraded silane stored at room temperature for 18 months, produces a veneer that looks perfect on delivery day and debonds under normal occlusal loading within one to three years.
Can zirconia veneers be bonded reliably?
Yes — but the standard glass-ceramic bonding protocol fails completely on zirconia because zirconia has no glass phase to etch. HF acid does nothing to its surface. Reliable bonding requires one of three validated approaches: zirconate-functional silanes, MDP (10-methacryloyloxydecyl dihydrogen phosphate) phosphate monomers that form chemical bonds with the zirconia oxide surface, or tribochemical silica coating (CoJet-type systems) that deposit a silica-modified layer onto the zirconia surface, after which conventional MPS silane application proceeds normally. Each route has trade-offs in equipment cost and workflow complexity, but all three achieve bond strengths sufficient for clinical service when executed correctly.
What is the practical difference between feldspathic porcelain and lithium disilicate?
Feldspathic porcelain’s 60–100 MPa flexural strength means it fractures under loads that lithium disilicate absorbs without incident. Lithium disilicate is roughly 3–4× stronger. For a dental laboratory running high CAD/CAM volume, lithium disilicate’s milling and pressing consistency also reduces remakes. Feldspathic porcelain remains the choice when an exceptional technician is hand-layering for a demanding anterior aesthetic case — its optical properties simply replicate natural enamel depth better than any pressed ceramic currently available. The decision is less about which material is superior and more about which material matches the lab’s workflow and the clinical risk profile of the specific patient.
How should dental laboratories specify and store silane coupling agents?
Specify a minimum 98.5% purity confirmed by gas chromatography. The hydrolyzable groups — methoxy or ethoxy — must be intact; any premature hydrolysis or condensation renders the product ineffective. Storage at 2–8°C in sealed containers away from moisture is not a recommendation but a shelf-life requirement. Working solution pH should fall between 4.5 and 5.5; outside that window, the hydrolysis-condensation balance shifts unfavorably. Use within 12 months of manufacture date, and require the supplier to provide a dated certificate of analysis, not just a safety data sheet.
What organosilicon products does SiliconChemicals supply for dental material manufacturing?
SiliconChemicals supplies MPS (3-methacryloxypropyltrimethoxysilane) and VTMO (vinyltrimethoxysilane) as core silane coupling agents for ceramic bonding systems and composite filler surface treatment. APTES (3-aminopropyltriethoxysilane) serves formulations requiring amine functionality for primer systems. Custom bifunctional silane blends are available for manufacturers who need tailored reactivity profiles without running their own synthesis. The portfolio extends into silicone polymers used as impression material bases and platinum catalyst systems for addition-cure silicone formulations — covering the full upstream chemistry stack that dental material producers typically source from multiple vendors.
How does sourcing silane coupling agents from China compare to European sources on quality?
China’s organosilicon industrial clusters — concentrated around production of chlorosilane intermediates — operate at a scale that supports the same purification, analytical, and quality management infrastructure as European producers. The assumption that geography correlates with purity is operationally outdated. SiliconChemicals provides full analytical dossiers including GC-MS purity profiles, NMR structural confirmation, and ISO 10993 biocompatibility compliance documentation upon request. Cost savings versus comparable European-sourced silanes typically run 25–40%, with the actual range depending on order volume, grade specification, and freight terms. Lead times on standard grades are competitive; custom blends require additional lead time for formulation validation. The practical question for a procurement manager is not where the molecule was made but whether the supplier can provide traceable batch documentation and consistent specification compliance — both of which are contractual requirements, not assumptions, in any responsible procurement relationship.
Why Material Quality Starts With the Chemistry Behind the Veneer: SiliconChemicals’ Role in the Supply Chain
Every section of this article has arrived at the same underlying conclusion through a different route. Feldspathic porcelain depends on silane coupling to achieve a durable resin bond across its silica-rich glass phase. Lithium disilicate requires carefully selected MPS-based primers to activate freshly etched surfaces before the adhesive cement contacts them. Zirconia — which has no etchable glass phase at all — relies entirely on phosphate-modified silane chemistry or 10-MDP/silane hybrid primers to develop a bond that survives oral loading cycles. Composite resin veneers need silane-treated filler particles at the manufacturing stage, and again at the surface when an indirect restoration is bonded chairside. The substrate changes; the dependence on organosilicon chemistry does not.

How SiliconChemicals’ Product Lines Map to Specific Application Nodes
The practical implication for dental material manufacturers and procurement teams is that organosilicon inputs appear at multiple, distinct stages of the production and clinical workflow — and each stage has its own specification requirements.
Gamma-methacryloxypropyltrimethoxysilane (MPS, also catalogued as MEMO or A-174 type) is the core silane for ceramic primer formulations and for surface treatment of silica, glass, and quartz fillers in composite paste manufacturing. Vinyltrimethoxysilane (VTMO) serves a complementary role in filler treatment where a simpler reactive anchor is sufficient and cost sensitivity is higher. Both require tight GC purity control — typically 97–99% minimum for dental applications — because hydrolysis byproducts and residual methanol affect both shelf life of finished primers and bond strength reproducibility in production QC.
Aminosilanes, particularly 3-aminopropyltriethoxysilane (APTES) and its trimethoxysilane equivalent, are the functional inputs for epoxy-based dental adhesive systems and some dual-cure cements where amine functionality accelerates curing and improves adhesion to metal oxide surfaces. Silicone polymers — specifically addition-cure vinyl-terminated polydimethylsiloxane systems catalyzed by platinum — underpin polyvinylsiloxane (PVS) impression materials, which remain the clinical standard for capturing preparation geometry before veneer fabrication. Platinum catalyst quality directly governs cure completeness, tear strength, and dimensional stability of the final impression; substandard catalyst lots produce soft spots or inhibited surfaces, translating into an inaccurate die and a veneer that requires remakes.
Quality Infrastructure That Procurement Managers Can Audit
SiliconChemicals operates under ISO 9001:2015 certified production. Each batch ships with a certificate of analysis reporting GC purity, refractive index, density, and functional group content (typically measured by hydrolysis titration for alkoxysilanes). REACH registration is maintained for EU-destined material, removing a common compliance bottleneck for European dental material manufacturers. These are not marketing claims — they are the minimum documentation a responsible procurement specification should require from any organosilane supplier.
Silicone-modified coupling agents such as MPS improve ceramic-resin bond durability by 30–60% compared to untreated controls in accelerated aging tests.True
This range is consistent with published ISO TR 11405-aligned bond strength studies comparing silanized vs. non-silanized ceramic surfaces under thermocycling protocols.
Partnership Structure for Dental Material Manufacturers
For manufacturers developing or reformulating veneer systems, SiliconChemicals offers sample kits of dental-grade organosilanes, joint formulation development support, and application notes covering primer concentration, hydrolysis conditions, and storage stability. Twelve-month pricing agreements are available, which matters when production planning requires stable raw material costs across a product cycle.
Export capability covers customers in Germany, Italy, and France across Europe; the United States and Canada in North America; South Korea, Japan, and Thailand across Southeast Asia; and buyers throughout the Middle East. DDP and CIF terms are available for key markets, reducing logistics complexity for first-time qualification orders.
Selecting the best veneer material is genuinely a multidimensional clinical and technical decision — one this article has worked through substrate by substrate. But regardless of which material wins that decision for a given indication, the organosilicon chemistry that makes it bond reliably and survive in the oral environment is sourced upstream, often invisibly, from a supplier whose batch consistency either supports or undermines every clinical outcome downstream. R&D teams, procurement managers, and dental lab owners are invited to request silane selection guidance, analytical data sheets, or initiate a supply qualification process directly with SiliconChemicals’ technical service team.














