
Zirconia crowns debond at the worst possible moment — during function, under load, often within the first two years of cementation. When that happens, the clinical cost is a remade crown, a disrupted schedule, and a patient who questions the entire treatment. The financial hit runs deeper than chair time: repeated remakes erode margins, and in high-volume prosthetic workflows a 5–10% debond rate can quietly consume a significant share of lab and material budget. The root cause is almost never the crown itself. It is an adhesive protocol that ignores zirconia’s chemistry — specifically its near-inert oxide surface that conventional resin cements cannot grip without deliberate surface activation.
The best material to bond zirconia crowns is an MDP-containing resin cement used alongside a dedicated MDP-based zirconia primer. MDP (10-methylenedecyl dihydrogen phosphate) forms a chemical bond with the zirconia oxide surface that silane alone cannot achieve. Combined with air-abrasion surface preparation, this approach consistently delivers bond strengths in the 15–35 MPa range — compared with 5–12 MPa when no surface treatment is used.
That range of 15–35 MPa is not academic noise. It is the difference between a cementation that survives years of occlusal cycling and one that fails before the patient’s next recall appointment. What drives performance to the high end of that range — and what collapses it to the low end — comes down to a sequence of decisions around surface preparation, primer chemistry, and cement selection that most protocols still get wrong.

Resin Cement Categories Ranked for Zirconia: Self-Adhesive, Conventional, and Dual-Cure Options Compared
Not all resin cements perform equally against zirconia’s chemically inert oxide surface. Choosing the wrong category is one of the most common causes of early crown debonding — a failure that looks like a cementation error but is actually a material science mismatch made at the point of purchase.
Self-Adhesive Resin Cements
Self-adhesive cements (the RelyX Unicem class) are the most operator-friendly option on the market, and that convenience comes with a real bond-strength penalty on zirconia. These materials rely on acidic functional monomers — typically methacrylate phosphates — to simultaneously condition tooth structure and initiate bonding in one step. The problem is that the cement’s own buffering chemistry neutralizes those acidic groups during the mixing and setting reaction. By the time the cement contacts zirconia, the monomers capable of chelating with Zr⁴⁺ surface ions have already been spent. Reported bond strengths for self-adhesive cements to untreated or air-abraded zirconia typically fall in the range of 8–14 MPa, depending on air-abrasion protocol, storage conditions, and thermocycling duration in the study design. That range is marginally acceptable for low-occlusal-load anterior restorations with good ferrule, but it is routinely insufficient for posterior crowns under heavy parafunction.
Self-adhesive resin cements provide equivalent long-term bond strength to zirconia as MDP-primer systemsFalse
Published in-vitro meta-analyses consistently show self-adhesive cements bonding to zirconia at 8–14 MPa versus 22–35 MPa for MDP-primer/conventional resin cement systems. The neutralization of acidic monomers during self-cure prevents effective phosphate ester chelation with Zr⁴⁺ ions.
Conventional Resin Cements with Separate MDP Primer
This is the highest-performing category for zirconia. Cements in the Panavia F 2.0 class work through a two-step process: first, an MDP-containing primer is applied to the air-abraded zirconia surface, where the phosphate ester group of the MDP monomer forms a coordinate covalent bond — chelation — with exposed Zr⁴⁺ ions. The methacrylate tail of the MDP molecule then co-polymerizes with the resin cement matrix during cure. This creates a durable chemical bridge between inorganic oxide surface and organic resin. Bond strengths reported in peer-reviewed in-vitro studies range from 22–35 MPa, with the upper end dependent on primer MDP concentration (optimal around 15–20 wt%), air-abrasion particle size (50-micron alumina is standard), and adequate primer contact time before cement placement.
Dual-Cure Resin Cements
Dual-cure formulations matter most in two specific scenarios: deep preparations where the curing light intensity drops below effective polymerization threshold, and monolithic high-opacity zirconia where light transmission through the crown body is negligible. A purely light-cured cement under a 1.5 mm full-contour zirconia crown will be substantially undercured at the cement-tooth interface. Dual-cure cements use a chemical initiator (typically an amine-peroxide redox pair) that continues polymerization in the dark. One operational warning: the oxygen inhibition layer that forms at the zirconia-cement interface during light cure can compromise bond integrity if the chemical cure phase is insufficient. Mixing ratio accuracy and working time discipline are non-negotiable with dual-cure systems.
Comparative Bond Strength by Cement Class
| Cement Type | Surface Treatment | Mean Bond Strength (MPa) | Predominant Failure Mode |
|---|---|---|---|
| Self-adhesive resin | Air-abrasion only | 8–14 | Adhesive (cement-zirconia interface) |
| Conventional resin + MDP primer | Air-abrasion + primer | 22–35 | Mixed / cohesive in cement |
| Dual-cure resin + MDP primer | Air-abrasion + primer | 18–30 | Mixed |
| Glass ionomer | None practical | 3–8 | Adhesive / crown fracture |
| Zinc phosphate | None practical | 4–9 | Adhesive |
Glass Ionomer and Zinc Phosphate: Contraindicated
Both glass ionomer and zinc phosphate cements are contraindicated for all-ceramic zirconia restorations. Neither material forms chemical bonds with the zirconia surface. Glass ionomer’s fluoroaluminosilicate chemistry has no mechanism to interact with ZrO₂. Under occlusal loading, the cement film — typically 20–80 microns — experiences shear stress that exceeds its tensile strength well before clinical fatigue would threaten a properly bonded resin system. Crown fracture, not just debonding, becomes a real risk because the cement deforms preferentially and transfers stress directly to the ceramic.
Clinical Selection Logic
Restoration type, preparation geometry, occlusal zone, and workflow speed all drive the decision. Anterior veneered zirconia with adequate ferrule and low occlusal load: a self-adhesive cement is a defensible choice if workflow speed is the priority. Posterior full-arch implant-supported zirconia under heavy load or bruxism history: conventional resin cement with dedicated MDP primer is the only rational selection. Any preparation depth exceeding 5–6 mm, or any monolithic block where light transmission is visually questionable: specify a dual-cure system and verify your mixing protocol against the manufacturer’s pot-life data.
MDP Monomer: The Chemical Workhorse of Zirconia Adhesion and How [Silane Coupling Agents](https://siliconchemicals.com/silane-coupling-agents/) Complement It
How MDP Actually Bonds to Zirconia at the Atomic Level
10-Methacryloyloxydecyl dihydrogen phosphate — universally abbreviated MDP — is not simply a primer additive. It is a bifunctional molecule designed around a specific bonding problem. On one end sits the phosphate ester group, which carries two acidic P–OH moieties capable of both ionic interaction and covalent chelation with the Zr⁴⁺ ions and surface hydroxyl groups (Zr–OH) that populate a zirconia surface. That phosphate headgroup exchanges protons with the surface oxide, forming Zr–O–P linkages that are genuinely stable under aqueous oral conditions — not merely physical adsorption that reverses on hydration cycling.
The opposite end carries a methacrylate group, which co-polymerizes directly into the resin cement matrix during light or dual-cure activation. Between those two reactive termini sits the ten-carbon aliphatic spacer chain. That chain length is not arbitrary. Shorter analogues (four to six carbons) position the methacrylate group too close to the ceramic surface, creating steric crowding that reduces conversion efficiency. Longer chains introduce excessive hydrophobic bulk and reduce packing density at the interface. The C10 spacer sits in the practical optimum: enough conformational flexibility to let the phosphate headgroup orient correctly on the surface while keeping the methacrylate terminus accessible for radical polymerization.
Published in-vitro data consistently show that MDP concentration in primers follows a bell-curve relationship with bond strength. Performance rises from roughly 5–12 MPa (untreated or no-primer controls) into the 15–35 MPa range as MDP loading climbs toward 15–20 wt% — the range where surface coverage is dense enough for robust chelation without molecular crowding. Push concentration above 25 wt% and bond strength begins declining, because excess MDP plasticizes the adhesive layer: the unpolymerized phosphate-rich material acts as an internal lubricant, softening the interface instead of strengthening it. How sharp that decline is depends on the solvent system and the specific resin matrix, but the trend is reproducible enough to treat 15–20 wt% as a formulation target, not a minimum.
Why Conventional [Silane Coupling Agents](https://siliconchemicals.com/silane-coupling-agents/) Fall Short on Zirconia
3-Methacryloxypropyltrimethoxysilane (MPTMS, also called γ-MPS) has been the standard surface coupling agent for silica-based ceramics — feldspathic porcelain, leucite glass-ceramic, lithium disilicate — for decades, and it works reliably there because those surfaces present abundant Si–OH groups. The trimethoxysilane headgroup hydrolyzes to silanol (Si–OH) in the presence of water or alcohol, then condenses with the substrate’s Si–OH groups to form Si–O–Si covalent bonds.
Zirconia has no silicon in its surface chemistry. The surface presents Zr–OH and Zr–O–Zr species. MPTMS silanol groups have negligible chemical affinity for Zr–O–Zr bridges and only weak physisorption onto Zr–OH. The result is that conventional silane treatment on unmodified zirconia improves surface energy marginally but delivers minimal durable chemical bonding. Any initial adhesion improvement largely comes from wettability enhancement, which hydrolyzes away under thermocycling.
Standard silane primers developed for glass-ceramics perform equivalently on zirconia.False
Conventional MPTMS-based silanes rely on Si–O–Si condensation with silica surfaces. Zirconia surfaces present Zr–OH groups, not Si–OH, so the condensation mechanism cannot operate. Bond strength improvement from conventional silane alone on ZrO2 is minor and hydrolytically unstable.
Hybrid and Zirconia-Specific Silane Architectures
The more productive research direction grafts zirconia-reactive anchor groups onto a silane backbone. Phosphate-functionalized trialkoxysilanes and titanate-chelating silanes retain the trialkoxysilane hydrolysis-condensation tail — relevant for adhesive matrix integration — while replacing the silanol-to-silica mechanism with phosphate-to-zirconia or titanate-to-zirconia chelation that directly mimics MDP’s binding logic. Some sol-gel synthesis routes introduce Zr-chelating headgroups through controlled hydrolysis of zirconium alkoxide precursors co-condensed with methacrylate-functional alkoxysilanes, yielding bifunctional oligomers that bond strongly to ZrO2 and remain co-reactive with methacrylate resins.
This is precisely the chemistry space where specialty modified silicone and organosilane manufacturing intersects with dental materials science. The sol-gel processing conditions — alkoxide hydrolysis ratios, catalyst choice, water content, reaction temperature — that govern particle size and network connectivity in these zirconia-reactive silane systems are the same variables controlled in industrial specialty silane production. Formulation chemists sourcing trialkoxysilane precursors or phosphate-modified silane intermediates for dental primer R&D need raw material suppliers who understand hydrolysis kinetics, not just commodity purity specs.
Solvent System Selection and Shelf Stability
Solvent choice in MDP-containing primers affects both silane hydrolysis rate and product shelf life in ways that matter to anyone scaling from lab formulation to industrial supply. Acetone-based systems promote fast silane hydrolysis and good initial wetting but accelerate MDP degradation during storage, compressing practical shelf life to months rather than years at ambient temperature. Ethanol slows hydrolysis, extending stability, but may reduce wetting on low-energy contaminated surfaces. Water content is the most critical variable: enough to drive silane hydrolysis, not so much that it promotes premature MDP salt formation or silane self-condensation into inactive oligomers. Formulators sourcing silane precursors industrially should expect suppliers to characterize moisture content and alkoxy group purity, since either variable shifts directly into the hydrolysis equilibrium of the finished primer.
Surface Treatment Protocols That Maximize Bond Strength Before Cement Application
Getting the chemistry right with an MDP primer or a well-formulated resin cement is only half the equation. The zirconia surface presented to that cement determines whether you reach the upper end of the 15–35 MPa bond strength range or scrape along at the bottom. Surface preparation is where most adhesion failures are seeded — quietly, before the crown is ever seated.
Air-Abrasion with 50-Micron Alumina
The standard starting point is intraoral or laboratory air-abrasion using 50-micron Al2O3 particles at approximately 2.5 bar pressure for 10–15 seconds per surface quadrant. Done correctly, this shifts surface roughness (Ra) from roughly 0.2 µm on as-sintered zirconia to around 1.4 µm, and pushes surface energy from approximately 30 mJ/m² up to 55 mJ/m² — an over-80% improvement in wettability that directly translates to better primer and cement spread.
Standoff distance matters more than most operators realize. Hold the nozzle 10 mm from the surface. Drop to 5 mm and you concentrate impact energy enough to introduce surface micro-cracking in high-translucency (low-cubic-content) zirconia grades. Go beyond 15 mm and you lose the mechanical surface disruption that drives the Ra increase. Particle size also carries operational weight: 110-micron alumina cuts faster but creates surface damage that outweighs the roughness benefit, while 25-micron particles produce inadequate mechanical interlocking for most resin cements.

Sandblasting Versus Tribochemical Silica Coating
Conventional sandblasting with alumina roughens the surface mechanically but leaves it chemically identical — still zirconia, still silane-resistant. Tribochemical silica coating systems (the CoJet or Rocatec approach) go a step further by embedding SiO2 particles into the zirconia surface through kinetic energy transfer. The result is an artificial silica-rich layer, typically 10–30 nm thick, that conventional silane coupling agents can chemically react with through the standard Si–O–Si condensation mechanism.
Published in-vitro comparisons consistently show bond strength uplifts of 40–60% for tribochemical silica coating over sandblasting alone, depending on resin cement type and MDP content in the bonding system. For high-stress posterior restorations, this gap is clinically meaningful. The trade-off is equipment cost and the additional protocol step — factors that matter in a high-volume lab but less so in a prosthodontic specialty practice.
Hydrofluoric Acid: The Protocol That Actively Fails on Zirconia
Hydrofluoric acid etching is effective for improving zirconia crown bond strengthFalse
HF etching dissolves the glassy phase in feldspathic ceramics and glass-ceramics, creating micro-porosity that silane can penetrate. Zirconia is a crystalline polycrystalline oxide with no glassy phase. HF has nothing to dissolve, produces no usable surface texture, and risks surface layer damage that degrades mechanical properties. Clinicians applying HF to zirconia are following a protocol designed for a fundamentally different material class.
This misapplication is not rare in mixed-ceramic clinical settings where a single acid-etch step is the default. The consequence is predictable: bond strengths in the 5–8 MPa range regardless of the cement selected, followed by early crown debonding under occlusal load.
Laser Conditioning
Er:YAG and Nd:YAG laser conditioning creates micro-retentive surface topography without introducing alumina contamination — a real advantage when residual abrasive particles are a concern. Current evidence places bond strength outcomes roughly equivalent to air-abrasion at 2.5 bar. The method costs more in chair time and equipment and does not consistently outperform well-executed air-abrasion, so it remains a niche choice rather than a default workflow.
Ultrasonic Cleaning After Abrasion
This step is skipped more often than any other in the protocol, and the penalty is measurable. Residual alumina particles physically block adhesive resin from contacting the zirconia surface. Studies document a 15–20% bond strength reduction when post-abrasion ultrasonic cleaning is omitted. The correct sequence is 60–90 seconds in an ultrasonic bath with 96% isopropanol or distilled water, followed by oil-free air drying. Running a contaminated surface directly into primer application is one of the more reliable ways to underperform with an otherwise sound cement.
Temperature and Humidity During Primer Application
MDP and silane coupling agents both undergo hydrolysis-condensation reactions that are rate-dependent on temperature. In a laboratory environment below 18 °C, activation kinetics slow enough that a standard 60-second air-dry at room temperature leaves a meaningful fraction of the coupling agent unreacted at the time of cement placement. The practical rule: bring primers to room temperature (20–25 °C range), apply in a thin even coat, and enforce the full air-dry time even when workflow pressure pushes for shortcuts. Humidity above 70% accelerates unwanted silane self-condensation before surface bonding occurs, particularly relevant in humid manufacturing or clinical environments without climate control. A thin, activated primer layer on a properly prepared, clean surface at controlled temperature is where the upper end of the bond strength range becomes achievable.
Primer Systems for Zirconia: Formulation Ingredients, Application Techniques, and Quality Benchmarks
A zirconia primer is not a single-ingredient solution. It is a carefully balanced formulation where each component earns its place, and substituting or skimping on any one of them produces measurable bond degradation at the cement-zirconia interface.
Anatomy of a High-Performance Zirconia Primer
The adhesion monomer is MDP (10-methacryloyloxydecyl dihydrogen phosphate). Its phosphate group forms ionic bonds with zirconium oxide surface sites; its methacrylate tail co-polymerizes into the resin cement matrix. But MDP alone does not make a complete primer. You need a co-monomer matrix builder — HEMA at lower viscosity grades for single-bottle systems, BisGMA where higher cross-link density and film toughness are prioritized — to give the polymerized primer film enough mechanical integrity to transfer load across the interface rather than fracturing cohesively under occlusal stress.
The initiator package matters more than most formulators acknowledge. A photoinitiator system (camphorquinone plus amine co-initiator is standard) works well in thin primer films where light penetration is reliable. Redox initiator packages suit dual-cure contexts where the primer layer sits under an opaque crown and receives no meaningful light exposure. Choosing the wrong initiator type does not produce an obvious clinical failure immediately — it produces a weak, partially polymerized interface that creeps under cyclic loading over 12–24 months.
Organosilane completes the formulation. It is not decorative. Gamma-methacryloxypropyltrimethoxysilane (MPS, also written γ-MPS or MAPTMS) is the workhorse silane here: its trimethoxysilyl end hydrolyzes to silanol groups that condense with surface hydroxyls on zirconia, while its methacrylate end copolymerizes with MDP and the co-monomer matrix. The net effect is improved wettability — surface energy on air-abraded zirconia climbs from roughly 30 mJ/m² to around 55 mJ/m² after proper silane conditioning — plus a measurable increase in cross-link density within the primer film itself.
Silane Raw Material Quality: Where Industrial Sourcing Directly Affects Clinical Outcomes
Formulators sourcing MPS or specialty silane variants for dental primer production need to specify to their supplier, not just assume. Minimum purity should be ≥99% by GC. Methoxy content must meet stoichiometric specification because under-methoxylated silane hydrolyzes incompletely, leaving unreacted silyl groups that act as weak points. Residual chloride below 10 ppm is non-negotiable — chloride contamination accelerates hydrolytic degradation of the silane film, shortening shelf life and reducing bond durability in the wet oral environment. Accelerated hydrolysis stability testing (typically 40°C/75% RH for 30 days with viscosity and turbidity monitoring) should be part of the incoming raw material acceptance protocol, not an afterthought.
Residual chloride above 10 ppm in silane raw materials accelerates hydrolytic degradation of the cured primer film.True
Chloride ions promote acid-catalyzed hydrolysis of Si-O-C and Si-O-Zr bonds at the interface, reducing long-term bond durability — well documented in silane surface chemistry literature.
Batch-to-batch consistency in silane intermediates directly determines whether a primer formulation hits its bond strength target lot after lot. A single off-spec batch can shift a validated formulation below the clinical threshold of 15–20 MPa that reliable cementation requires.
Single-Bottle vs. Two-Bottle Systems: A Real Trade-Off
Single-bottle primers are convenient. They are also chemically compromised by design. MDP and silane compete for the same surface hydroxyl sites on zirconia, and in a pre-mixed solution, partial MDP-silane interaction in storage reduces the active concentration of both species. Two-bottle systems — MDP solution and silane solution applied sequentially — preserve the full activity of each component. Published in-vitro data consistently show 5–10 MPa higher bond strengths for sequential application versus premixed single-bottle alternatives, depending on cement type and zirconia grade.
The convenience argument is real in a busy clinical setting. The performance argument favors two-bottle systems for long-span bridges or implant-supported frameworks where any bond failure has severe consequences.
Application Technique: Small Errors, Large Consequences
Number of coats: a single thin coat often leaves incomplete coverage on rough air-abraded surfaces; two coats applied with 20–30 seconds of active scrubbing between them reliably fills surface microporosities. Passive application — dabbing primer on and letting it sit — underperforms active agitation, which mechanically works the low-viscosity primer into surface irregularities.
Evaporation time before light-curing or cement application is critical and consistently underestimated. Residual solvent (ethanol or acetone carrier) dilutes monomer concentration at the zirconia interface if evaporation is cut short. Thirty to sixty seconds of gentle air-drying at low pressure, not blasting with high-pressure air that blows the primer film off the surface, achieves adequate solvent removal without disturbing film continuity.
Overwetting is the opposite failure mode: excess primer pooling in intaglio surface recesses produces a thick, poorly cross-linked film with lower modulus than optimally thin primer layers. Optimal film thickness is in the range of a few micrometers — enough for full surface coverage, thin enough to not act as a stress-absorbing compliant layer that reduces load transfer to the cement.
Shelf life for formulated primers typically runs 18–24 months under refrigerated storage (2–8°C), shorter at room temperature. For raw silane intermediates in bulk, moisture ingress is the primary degradation mechanism. Sealed containers with nitrogen blanketing and moisture-barrier packaging are standard requirements when sourcing from qualified industrial manufacturers.
Translucent vs. High-Strength Zirconia Generations: How Material Evolution Changes the Bonding Strategy
The zirconia your lab milled five years ago is not the same material in today’s ultra-translucent disc. Yttria content has climbed, cubic phase fraction has grown, and the clinical bonding assumptions that worked for first-generation crowns can quietly fail on modern esthetic restorations.
Three Generations, Three Different Bonding Realities
3Y-TZP (3 mol% yttria, tetragonal zirconia polycrystal) remains the workhorse for high-load posterior bridges and implant frameworks. Flexural strength sits in the 900–1200 MPa range depending on powder processing and sintering cycle. The microstructure is predominantly tetragonal, dense, and opaque. Surface hydroxyl group density is relatively high, which means MDP monomer has adequate reactive sites for chelation. Achievable resin cement bond strengths with a proper MDP primer run 20–35 MPa; without primer, that drops to the 5–12 MPa range — a gap wide enough to determine clinical survival.
4Y-PSZ and 5Y-PSZ (4–5 mol% yttria, partially stabilized with increasing cubic phase) were developed specifically to raise light transmission for anterior esthetics. Translucency increases substantially, but flexural strength falls to roughly 700–900 MPa for 4Y and 500–700 MPa for 5Y formulations, depending on manufacturer sintering parameters and grain size. The critical point: as yttria content rises and cubic phase fraction increases, surface hydroxyl group density decreases. Fewer hydroxyl sites mean MDP chelation is less efficient, and published in-vitro data consistently show lower bond strength ceilings for 5Y-PSZ compared to 3Y-TZP under identical primer protocols.
This creates an uncomfortable paradox. The crown that is most mechanically vulnerable — 5Y-PSZ with its lower bulk strength — simultaneously demands the strongest resin cement interface for fracture resistance, yet presents a surface that is harder to bond chemically. That combination demands rigorous surface preparation, not a relaxed one.

CAD/CAM Milling Residues: The Overlooked Bond Killer
Multi-layer gradient discs introduce an additional contamination variable. Milling lubricants, coolant residues, and machining debris embed into the zirconia surface during wet-milling. Sintering atmosphere contaminants — residual carbon from binder burnout or furnace oils — can deposit on grain boundaries. Bond strength studies consistently show that contaminated 5Y-PSZ surfaces tested without decontamination produce bond values in the 8–15 MPa range even with MDP primers, compared to 18–28 MPa on properly cleaned surfaces. The decontamination protocol matters: ultrasonic cleaning in isopropanol for 3–5 minutes, followed by steam cleaning or air-abrasion with 30–50 µm alumina at 0.1–0.2 MPa, removes both organic residues and loosely adherent particles before primer application.
Milling lubricant residues on zirconia surfaces can reduce MDP primer bond strength by 30–50% even when all other protocol steps are correctly followed.True
Organic contamination blocks MDP access to zirconia hydroxyl groups, reducing chelation efficiency. Multiple in-vitro studies confirm significant bond strength reduction when decontamination is omitted, regardless of primer type.
Pre-Sintered vs. Post-Sintered Surface Treatment
Some digital workflows propose air-abrading or chemically treating zirconia in its pre-sintered (chalk-stage) form before the 1400–1500°C sintering cycle. The logic is easier material removal and better particle embedding. The problem is that sintering recrystallizes the surface, eliminating any mechanical roughness created earlier and potentially altering hydroxyl group chemistry. Post-sintering surface treatment is therefore the only reliable approach for mechanical preparation. The sintering cycle itself is not optional or adjustable for bonding purposes — crystallographic transformation is complete, grain growth is fixed, and the surface you treat with primer is the surface the cement actually contacts.
Matching Zirconia Generation to Clinical Indication and Bonding Protocol
| Clinical Indication | Recommended Zirconia Generation | Minimum Surface Prep | Cement Choice |
|---|---|---|---|
| Posterior full-arch bridge | 3Y-TZP | Air-abrasion + MDP primer | Dual-cure resin cement |
| Posterior single crown, high occlusal load | 3Y-TZP or 4Y-PSZ | Air-abrasion + MDP primer | Dual-cure or self-adhesive with MDP |
| Anterior single crown, esthetic priority | 4Y-PSZ or 5Y-PSZ | Decontamination + air-abrasion + MDP primer | Dual-cure resin cement, light shade |
| Implant-supported crown (screw-access) | 3Y-TZP | Air-abrasion + MDP primer | Resin-modified glass ionomer or dual-cure |
| Anterior veneer-thickness restoration | 5Y-PSZ multilayer | Full decontamination protocol + high-concentration MDP primer | Dual-cure resin cement only |
Yttria content, cubic phase fraction, and contamination history all converge at the bonding interface. Treating a 5Y-PSZ multilayer disc with the same casual protocol appropriate for a chunky 3Y posterior crown is one of the more reliable ways to see a returned restoration within two years.
Long-Term Bond Durability: Thermocycling, Hydrolytic Aging, and Clinical Survival Data
Knowing that a bond tests well on the day of cementation is necessary but not sufficient. What procurement managers and formulation chemists actually need is evidence that the bond holds five, eight, ten years into clinical service — through thousands of thermal excursions, constant salivary moisture, and the mechanical fatigue of mastication. That evidence base exists, and it draws a sharp line between MDP-containing adhesive systems and everything else.
Thermocycling as an Accelerated Aging Proxy
ISO 11405 is the accepted framework for simulating intraoral thermal stress: specimens cycled between 5°C and 55°C, 10,000 cycles, with dwell times standardized at each extreme. Ten thousand cycles approximates roughly 5–7 years of clinical thermal loading, though the precise equivalency depends on patient diet, beverage temperature habits, and cycle dwell time used in the specific protocol. This range matters when you see a manufacturer cite “10,000-cycle durability” — the absolute number means little without knowing dwell time and transfer speed between baths.
After completing ISO 11405 thermocycling, MDP-containing primer-cement systems typically retain 75–90% of their initial bond strength to zirconia. Non-MDP self-adhesive resin cements — which rely primarily on carboxylate or phosphate groups with weaker Zr–O coordination chemistry — drop to 30–50% retention under identical conditions. The gap widens as cycles increase. At 5,000 cycles the difference is already detectable; by 10,000 it is clinically decisive.
Hydrolytic Degradation: The Chemistry of Slow Bond Failure
Water is the primary long-term enemy of resin-to-zirconia bonds. The degradation pathway runs through two simultaneous mechanisms. First, water uptake by the BisGMA/TEGDMA resin matrix causes volumetric swelling and plasticizes the polymer network, progressively reducing the elastic modulus of the cement film. Second — and more damaging — ester linkages in BisGMA are susceptible to hydrolytic scission under sustained aqueous exposure, breaking polymer chain continuity and accelerating cohesive weakening.
MDP slows both mechanisms. Its phosphate-Zr coordination bond is hydrolytically stable at physiological pH (roughly 6.5–7.5), forming a calcium- and zirconium-reactive interface that resists water-mediated displacement. High MDP concentration in the primer — the 15–20 wt% range identified in in-vitro studies as optimal — creates a denser chemical bridging layer that limits water ingress at the cement-zirconia interface. Formulators who reduce MDP content to cut costs are trading long-term bond stability for a short-term material savings that can show up as clinical debonding at year four or five.
What Clinical Survival Data Actually Shows
Ten-year retrospective data on zirconia crowns cemented with MDP-based adhesive protocols consistently reports survival rates in the 93–96% range. Comparable restorations luted with conventional glass ionomer or non-MDP resin cements fall in the 78–85% range over the same interval. These figures come from multiple independent clinical cohort studies and systematic reviews published in journals covering prosthodontics and dental materials — the exact rates vary by study design, tooth position, and operator protocol, but the directional separation between MDP and non-MDP groups is consistent across the literature.
Failure Mode Analysis: Where Bonds Actually Break
Scanning electron microscopy of retrieved failed restorations cemented with correctly applied MDP primer tells a consistent story: fracture runs cohesively through the cement layer, not at the zirconia surface. The zirconia interface itself remains intact. This is the validation that the chemistry is working — failure moves to the weakest link, which is the bulk resin, not the adhesive junction. When MDP primer is skipped or applied incorrectly, SEM shows adhesive failure at the zirconia surface, leaving clean ceramic and confirming that no chemical bonding was ever established.
Industrial Raw Material Implications
This durability evidence has direct consequences for how dental adhesive formulators specify raw materials. Long-term hydrolytic stability of the silane coupling agent and MDP intermediate is not a marketing claim — it is a qualification requirement. Formulators need accelerated aging data on the raw silane: contact angle stability after water immersion, bond retention curves after simulated hydrolytic exposure, and batch-to-batch consistency in reactive group concentration. SiliconChemicals supplies silane intermediates used in dental adhesive formulation with accelerated aging characterization data, giving formulators the documentation needed to substantiate their own durability claims to regulatory bodies and purchasing customers.
MDP-containing zirconia primer systems retain 75–90% of initial bond strength after ISO 11405 thermocycling (10,000 cycles), compared to 30–50% for non-MDP self-adhesive cements.True
This range is consistent with published in-vitro studies using standardized thermocycling protocols. Retention values depend on cement formulation, MDP concentration, and surface treatment protocol applied before cementation.
Implant-Supported Zirconia Crowns and Full-Arch Zirconia Restorations: Bonding to Titanium and Zirconia Abutments
Implant-supported zirconia restorations introduce a complication that tooth-supported crowns simply do not have: two chemically distinct bonding interfaces operating simultaneously under the same occlusal load. The crown’s internal surface is zirconia. The abutment’s external surface is either titanium alloy or zirconia. Each requires a different surface chemistry strategy, and a protocol that optimizes one while neglecting the other will eventually fail at the weaker interface — typically under fatigue loading rather than a single high-force event.
The Titanium Abutment Interface: TiO2 Chemistry and MDP’s Dual Role
Titanium abutments are not bare metal. They carry a passive TiO2 oxide layer, 2–10 nm thick depending on surface finishing and sterilization history. This oxide layer is actually favorable for adhesion chemistry: the phosphate group in MDP monomer forms coordinative bonds with titanium oxide in the same way it bonds to zirconia’s ZrO2 surface. Published work consistently shows that MDP-containing primers raise bond strength to titanium surfaces to ranges of 18–28 MPa, depending on titanium alloy grade, surface roughness, and thermocycling conditions.
MDP-based primers designed for zirconia bonding also develop meaningful chemical adhesion to titanium oxide surfaces, allowing a single primer to serve both interfaces in implant cementation.True
MDP's phosphate group coordinates with both ZrO2 and TiO2 via acid-base interactions with surface metal oxide sites. Multiple in-vitro studies confirm measurable bond strength gains on titanium when MDP-containing primers are applied, though titanium-specific sandblasting with 50-micron alumina or dedicated TiO2 primers can further optimize the titanium interface.
Practically, this means a well-formulated MDP primer at 15–20 wt% MDP concentration can serve both surfaces without switching products mid-protocol — a real workflow advantage in a busy implant placement session. Air-abrading the titanium abutment external surface with 50-micron alumina before seating raises surface energy substantially and removes organic contamination; this step is straightforward in the laboratory but must be done before abutment placement, never after.
Zirconia Abutments: The Intraoral Priming Problem
When the abutment itself is zirconia, the chemistry challenge is identical to bonding a zirconia crown — but the clinical options are narrower. A seated zirconia abutment cannot be air-abraded in the mouth without risking soft-tissue and implant-fixture contamination. Intraoral protocol therefore relies on phosphoric acid or specific zirconia-reactive decontaminants, followed by thorough application of an MDP-based primer. Contamination from saliva, blood, or crevicular fluid in the seconds between priming and crown seating can reduce effective bond strength by 30–50%, which is why immediate isolation and a defined working-time protocol are not optional.
Cement-Retained vs. Screw-Retained: Viscosity and Metering Matter
Cement-retained implant crowns demand tighter control over cement film thickness than tooth-supported crowns. Excess cement extruding subgingivally around implants is a well-documented cause of peri-implantitis, with consequences ranging from bone loss to implant failure. A dual-cure resin cement with controlled, lower viscosity — typically 20–60 Pa·s at placement viscosity depending on formulation — allows more predictable film thickness control and easier removal of excess before cure. Some clinicians apply cement only to the internal crown surface margins rather than flooding the full internal volume, deliberately leaving the central area uncemented to reduce excess extrusion. The point is that cement viscosity specification is a clinical decision, not merely a product characteristic.
Provisional Cementation and Contamination Risk
Temporary cements on implant abutments create a surface contamination problem that is easy to underestimate. Eugenol-containing temporary cements are well established as inhibitors of resin polymerization at the interface. Even eugenol-free temporary cements leave a residue layer that interferes with MDP primer adhesion unless removed with isopropyl alcohol scrub followed by a clean pumice polish — a step that is frequently skipped under time pressure. Any residual temporary cement at the bonding surface is effectively a bond-strength reduction layer.
Full-Arch Monolithic Zirconia: Where Bond Failure Has System-Wide Consequences
Full-arch monolithic zirconia bridges on multi-unit abutments amplify every bonding variable. Passive fit is prerequisite: internal stress from a misfit framework loads the cement interface continuously before the patient bites down at all. Bond strength requirements for single implant crowns (often cited as a minimum threshold of 10–15 MPa clinically) are inadequate as a benchmark for full-arch cases where cantilever forces and torque moments at each abutment seat can be several times higher. When one cement interface fails in a full-arch case, the remaining interfaces absorb redistributed load — accelerating their own degradation. Retrievability is therefore not just convenient; in full-arch cases, designing for retrievability through screw-retention or low-retention temporary cement at one or more sites is a structural risk-management decision.
Industrial Supply Chain for Zirconia Bonding Raw Materials: Silanes, MDP Intermediates, and Specialty Monomers
Dental material formulators rarely think about where their silane coupling agents come from — until a batch fails incoming QC or a key supplier quotes a 16-week lead time. For anyone manufacturing zirconia primers, adhesive cements, or surface treatment kits at scale, the raw material supply chain is as consequential as the formulation chemistry itself.
Key Silane Inputs and Their Roles in Dental Adhesive Systems
Three organosilane intermediates dominate dental primer and cement formulations. 3-Methacryloxypropyltrimethoxysilane (MPS, also marketed as A-174) is the workhorse silane for zirconia and ceramic surface functionalization — its methacrylate group co-polymerizes with the resin matrix while the trimethoxysilyl end hydrolyzes and condenses onto oxide surfaces. 3-Glycidoxypropyltrimethoxysilane (GPS, A-187) appears in formulations where epoxy-functional coupling provides a different crosslink density or where the formulator is targeting compatibility with specific resin cement backbones. Vinyl-functional silanes serve more specialized roles: they appear in experimental and commercial primers where radical chain-transfer behavior is deliberately engineered, and in some self-adhesive cement formulations that prioritize rapid cure kinetics over maximum bond strength.
Each silane grade has purity specifications that genuinely matter at the clinical end. MPS used in dental applications typically requires GC purity above 97–98%, with residual methanol and hydrolyzed silanol species held below defined limits. Silanol content affects shelf stability and pot life; a batch with even 1–2% pre-hydrolyzed product will show shortened working time and inconsistent bond strength results in finished primers. NMR structural confirmation — both ¹H and ²⁹Si — is the realistic standard for qualifying a new supply source, not GC alone.

MDP Monomer: Synthesis Pathway and Purity Requirements
MDP (10-methacryloyloxydecyl dihydrogen phosphate) is synthesized by phosphorylating 10-hydroxydecyl methacrylate using either phosphorus oxychloride or polyphosphoric acid. The POCl₃ route gives tighter control over the mono-phosphate to di-phosphate ratio — the mono-ester is the active bonding species, and excessive di-phosphate content suppresses bond strength by competing for zirconia surface sites without contributing productive adhesion. Published in-vitro data consistently shows optimal chemical bonding at MDP concentrations of 15–20 wt% in primer formulations; above that range, competitive adsorption effects and osmotic stress during aging begin to reduce rather than improve long-term durability.
For dental-grade MDP, formulators should specify: mono-ester content above 85% of total phosphate species, residual POCl₃ or phosphoric acid byproducts below 0.5%, and heavy metals (Pb, Cd, As) below 10 ppm — a threshold directly relevant to the ISO 10993 biocompatibility documentation pathway that finished-device manufacturers must navigate. Color (APHA below 30) and acid value consistency batch-to-batch matter more than many buyers realize; acid value drift of even ±5 mg KOH/g shifts the primer’s pH and alters surface-conditioning behavior on zirconia.
Chinese organosilane manufacturers can match Western European or Japanese suppliers on technical purity for dental-grade MPS and GPS silanesTrue
Multiple Chinese producers in Zhejiang and Jiangsu now operate with GC purity certifications, NMR QC protocols, and ISO 9001-compliant QA systems. The technical gap that existed a decade ago has narrowed substantially for commodity and mid-complexity silanes, though ultra-specialty phosphate-functional intermediates still require careful supplier qualification.
China’s Organosilicon Industrial Cluster Advantage
Zhejiang, Jiangsu, and Shandong province host integrated organosilicon production clusters where chlorosilane feedstock, siloxane intermediates, and downstream specialty silanes are manufactured within tight geographic and logistical networks. That integration compresses cost and lead time in ways that are structurally difficult for Western European or Japanese stand-alone specialty chemical producers to match. For a commodity silane like MPS, cost-per-kilogram from a qualified Chinese supplier typically runs 30–55% below equivalent European quotes, depending on order volume and specification tier — and that gap widens for multi-tonne annual contracts.
For dental material formulators running development batches, minimum order quantities for custom-specification silane intermediates from Chinese manufacturers typically range from 25–100 kg, with lead times of 4–8 weeks for non-stock specifications. Standard-grade MPS and GPS are usually available ex-stock or within 2–3 weeks. The practical risk is not quality — it is documentation completeness. Regulatory affairs teams at dental device companies need Substance Safety Data Sheets, Certificate of Analysis with batch traceability, and ideally a Drug Master File-equivalent technical dossier to support their 510(k) or CE-mark submissions. Not every Chinese supplier maintains that documentation stack as a standard deliverable; it should be a pre-qualification requirement, not an afterthought.
SiliconChemicals’ Position in the Dental Material Supply Chain
SiliconChemicals supplies methacrylate-functional silanes including MPS, phosphate-modified silane intermediates, and specialty silicone polymer platforms that serve as direct raw material inputs for dental primer and cement formulators. The company’s position within China’s organosilicon industrial clusters gives it feedstock cost advantages that translate into competitive landed pricing for global customers, while its technical support capability — formulation guidance, application testing data, and regulatory documentation support — addresses the gap that historically made buyers hesitate to qualify Chinese silane suppliers for dental applications.
For procurement managers building dual-source strategies, the practical framework is straightforward: qualify a primary Western supplier for regulatory continuity on existing products, and run a parallel qualification of a Chinese source for cost leverage and supply resilience. For MPS and GPS at dental grade, that qualification process — NMR confirmation, GC purity, heavy metal panel, accelerated stability at 40°C/75% RH over 12 weeks — typically takes 3–5 months and is a one-time investment that pays back within the first or second commercial order.
Frequently Asked Questions About Bonding Zirconia Crowns
Can you use glass ionomer cement to bond zirconia crowns?
Not recommended, and in most full-ceramic zirconia cases, a poor clinical decision. Glass ionomer bonds to tooth structure through ionic exchange with hydroxyapatite — a mechanism that simply does not translate to a dense, oxide-based ceramic surface. Bond strength values for conventional glass ionomer to unprimed zirconia typically fall below 5 MPa, well under the 15–35 MPa range achievable with MDP-containing resin cements and proper surface preparation. The more serious consequence is microleakage: glass ionomer’s relatively high solubility in oral fluids creates a progressive ingress pathway at the cement-crown interface, leading to secondary caries, sensitivity, and eventually debonding. Reserve glass ionomer for its actual strengths — metal-based restorations and situations demanding fluoride release over retention.
Does zirconia need sandblasting before cementation?
Yes, for the vast majority of clinical protocols. Air-abrasion with 50-micron alumina at 0.1–0.2 MPa air pressure raises zirconia surface energy from roughly 30 mJ/m² to around 55 mJ/m², improving wettability by more than 80% and creating micro-mechanical retention that complements chemical bonding. The practical consequence: bond strength climbs substantially and cement film adhesion becomes far more uniform. The exception is CAD/CAM blocks or pre-sintered zirconia units that arrive with factory-applied primer coatings already integrated during manufacturing. Sandblasting those surfaces can strip the coating without providing equivalent benefit. Check the manufacturer’s technical data sheet before reaching for the air-abrasion unit.
What is the difference between a zirconia primer and a universal adhesive for zirconia bonding?
The label “universal adhesive” promises broad compatibility but does not guarantee effective zirconia bonding. The key variable is MDP concentration — commercial zirconia primers typically contain 10–30 wt% MDP, and in-vitro studies consistently identify 15–20 wt% as the range where chemical bonding to ZrO₂ surfaces peaks. Universal adhesives marketed for multiple substrates often sit at the lower end of that range, or omit MDP entirely in favor of other functional monomers that lack the phosphate-chelation mechanism specific to zirconia oxide surfaces. When evaluating a product, request the technical data sheet and look for explicit MDP content and an ISO 29022 or equivalent zirconia bond strength test result. If that data is absent, treat the product as unverified for zirconia.
How long does a properly bonded zirconia crown last?
Clinical survival data across multiple cohort studies places 10-year survival at 93–96% when MDP-based cementation is combined with adequate surface preparation and sound preparation design. That range narrows or widens depending on parafunctional habits (bruxism substantially increases debonding and fracture risk), occlusal preparation height (short preparations under 4 mm increase torque forces on the cement layer), and abutment surface area. Crowns on endodontically treated teeth with post-and-core buildup introduce additional stress concentration. A well-bonded crown with a textbook protocol and a cooperative patient will consistently reach the top of that range.
Is silane alone enough to bond zirconia without MDP?
No. This is a common and consequential formulation error. Silane coupling agents work by bridging an organic resin matrix to a silica-containing surface through Si–O–Si covalent linkages. Zirconia contains no free silica phase at its surface — it is a crystalline oxide ceramic. Silane has no chemical anchor point on ZrO₂. MDP provides that anchor through phosphate chelation to zirconium ions. The two chemistries are synergistic: silane improves the organic–inorganic interface where silica is present (such as in silica-coated zirconia protocols), while MDP handles the direct oxide bonding. Using silane alone on unmodified zirconia produces bond strengths comparable to no treatment at all.
Silane alone produces clinically adequate bond strength to unmodified zirconiaFalse
Zirconia lacks a silica surface phase, so silane coupling agents have no chemical anchor on ZrO₂. MDP phosphate chelation is required for chemical bonding; silane complements but cannot replace it.
What happens if the zirconia crown is contaminated with saliva or blood before cementation?
Protein adsorption is the problem. Salivary proteins and blood components physically occupy the ZrO₂ surface sites where MDP phosphate groups need to chelate. Bond strength drops measurably — some studies report reductions of 30–50% from contaminated versus clean surfaces. The decontamination protocol: apply 37% phosphoric acid for 15 seconds, rinse thoroughly, air-dry, then reapply the zirconia primer fresh. Do not simply re-dry with air and proceed. The acid displaces adsorbed proteins and re-exposes oxide bonding sites.
Can the same cement used for lithium disilicate be used for zirconia?
The resin cement itself often overlaps — dual-cure resin cements work for both. What differs fundamentally is the surface treatment and primer protocol. Lithium disilicate responds to hydrofluoric acid etching and silane coupling because it contains a silica glass phase. Zirconia does not, so HF etching provides no benefit and silane alone is insufficient. Applying a lithium disilicate protocol to zirconia — HF etch, silane, resin cement — produces bonds at the lower end of the untreated range. The cement is reusable across both substrates only when the primer and surface prep protocol is correctly switched for each material.
What raw material silanes does SiliconChemicals supply relevant to dental adhesive formulation?
SiliconChemicals manufactures methacrylate-functional silanes — including 3-methacryloxypropyltrimethoxysilane (MPS/A-174 type) — used as cross-linking and wetting agents in primer formulations where a silica co-phase or silica-coated ceramic substrate is involved. For formulators working on phosphate-silane hybrid systems, SiliconChemicals also supplies phosphate-modified organosilane intermediates suited for integration with MDP in multi-functional zirconia primer matrices. These materials are produced under tightly controlled purity specifications, because residual hydrolysis byproducts in silane batches directly affect shelf life and in-use bond strength consistency of finished primers. Industrial buyers sourcing for dental adhesive production should request certificate of analysis data covering silanol content, methoxy residuals, and viscosity range — all of which affect formulation reproducibility at scale.
Practical Decision Framework: Selecting the Optimal Bonding System for Every Zirconia Crown Scenario
Every section of this article builds toward one clinical or formulation moment: you are standing at the bench, or writing a material specification, and you need to make a call. The table and checklists below consolidate the evidence into tools you can use without flipping back through pages of chemistry.
Decision Matrix by Clinical Scenario
| Clinical Scenario | Zirconia Generation | Surface Treatment | Primer Type | Cement Type | Key Precaution |
|---|---|---|---|---|---|
| Posterior single crown (high load) | 3Y-TZP high-strength | Air-abrasion 50 µm Al₂O₃ + clean | MDP-containing primer, 15–20 wt% | Dual-cure resin cement | Verify occlusal clearance ≥ 0.5 mm for adequate film thickness |
| Anterior single crown (esthetic) | 5Y-TZP or multi-layer | Air-abrasion (low pressure, 25–30 µm) + clean | MDP primer, color-stable formulation | Light-cure or dual-cure, shade-matched | Over-abrasion on translucent zirconia distorts optical properties |
| Implant-supported crown | 3Y or 4Y-TZP | Abutment-specific: Ti surface sandblast + Ceramic Primer on zirconia cap | MDP + silane combination primer | Self-adhesive or dual-cure resin cement | Two separate bonding interfaces — treat each independently |
| Full-arch bridge | 3Y-TZP (connector zirconia) | Comprehensive air-abrasion all bonding surfaces | Full-coverage MDP primer application | Dual-cure resin cement, low film thickness | Incomplete primer coverage at connector recesses is a leading failure site |
| High-translucency esthetic case | 5Y or 4Y-TZP | Gentle air-abrasion 25 µm, no tribochemical silica coating | MDP primer only — silane alone insufficient | Dual-cure, low opacity shade | Skip HF entirely; silane without MDP yields unreliable bonds on this zirconia grade |
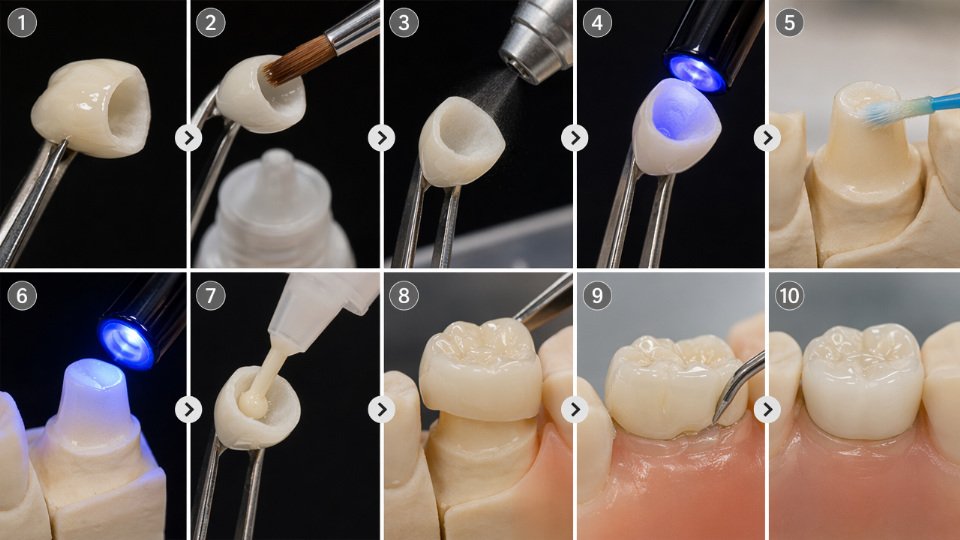
Step-by-Step Bonding Protocol for the Highest-Evidence Workflow
This sequence reflects the protocol with the strongest in-vitro and clinical survival support. Deviation at any step compounds error.
- Air-abrasion: 50 µm aluminum oxide, 0.2–0.28 MPa, 10 mm distance, 10–15 seconds per surface. Surface energy rises from roughly 30 mJ/m² to ~55 mJ/m², which translates directly to improved cement wettability.
- Ultrasonic cleaning: 99% isopropanol or distilled water, minimum 3 minutes. Removes alumina particles and contamination. Air-dry thoroughly.
- MDP primer application: Active scrubbing motion, 60 seconds, full surface coverage including margins. Air-dry 15 seconds — gentle stream, do not blast.
- Resin cement placement: Apply dual-cure cement to the crown inner surface immediately after primer. Delay beyond 60 seconds risks primer film degradation.
- Seating and initial cure: Seat with steady, even pressure. Remove gross excess before full light activation.
- Light activation sequence: Tack-cure 2–3 seconds to gel the margins, clean excess, then full activation 20–40 seconds per surface per manufacturer protocol for the specific cement thickness.
Six Red Flags That Guarantee Bond Failure
- Using hydrofluoric acid on zirconia. HF etches silica-based ceramics. Zirconia has no silica matrix to attack. You get surface contamination, not etching.
- Skipping primer entirely. Bond strength drops from a 15–35 MPa range to 5–12 MPa — roughly half to one-third of the clinically adequate value.
- Provisional cement contamination. Eugenol-containing temporaries suppress resin polymerization. Even trace residue at the margin is enough.
- Storing MDP primer above 25°C. Monomer hydrolysis accelerates sharply above this threshold; opened primer stored in a warm operatory drawer for six months is functionally degraded.
- Inadequate cement film thickness. Too thin and the cement fractures under occlusal load; too thick and seating is incomplete. Target film thickness depends on cement viscosity — confirm against the manufacturer’s spec sheet, typically 25–50 µm.
- Bonding without rubber dam or field isolation. Salivary contamination post-primer application requires the entire protocol to restart from cleaning.
Hydrofluoric acid etching improves bond strength to zirconia crownsFalse
HF acid is effective on silica-based ceramics such as feldspathic porcelain and lithium disilicate because it dissolves the silica phase, creating a micro-retentive surface. Zirconia is a polycrystalline oxide ceramic with no meaningful silica content, so HF produces no useful surface topography and instead leaves a contaminated surface that can actively impair bonding.
Cost-Benefit Reality for Dental Practices
A premium MDP-containing primer and matched dual-cure resin cement system costs roughly 2–4× more per placement than a basic self-adhesive cement used without dedicated primer. That differential amounts to a modest per-crown cost increase — the exact figure depends on regional pricing and kit size, but it is typically small relative to total crown fee. A debonded crown requiring recementation or replacement at three to five years carries direct material costs, laboratory fees, and chair time that can easily represent 30–60% of the original crown fee, depending on the clinical situation and whether a new crown is required. The economics favor the premium protocol decisively once failure probability is factored in.
Guidance for Dental Material Formulators and Industrial Buyers
When specifying raw materials for zirconia primer formulation, minimum performance benchmarks should include: MDP monomer purity ≥ 98%, acid value consistent with specification (batch-to-batch variation in phosphate content directly affects bonding chemistry), silane coupling agent hydrolysis stability at working dilution, and confirmed compatibility with photoinitiator systems used in the base resin. Supplier qualification should require certificate of analysis per batch, ISO 9001 manufacturing certification, and willingness to provide application development support — not just a data sheet.
SiliconChemicals supplies silane coupling agents and organosilicon intermediates relevant to dental adhesive formulation, including phosphate-functionalized silane precursors used in next-generation MDP-silane hybrid systems. Sample evaluation and technical consultation are available through direct inquiry; formulators should specify intended application, target substrate, and performance benchmarks when requesting samples so the technical team can recommend the appropriate intermediate.
What Is Coming Next in Zirconia Bonding Chemistry
Three directions are moving through academic development pipelines and will likely reach commercial formulation within the next five to ten years. Nano-structured surface treatments — including femtosecond laser texturing and anodization-derived surface topographies — create mechanical interlocking at a scale that complements chemical bonding rather than replacing it. Bio-inspired polydopamine adhesion layers, derived from mussel adhesion protein research, show early promise for creating a universally wettable intermediate layer on oxide ceramics without requiring abrasion. Phosphate-silane hybrid coupling agents combine the proven zirconia affinity of MDP-type phosphate groups with the silica network reactivity of conventional silanes in a single molecule, potentially simplifying primer formulation while extending bond durability. None of these are ready for routine clinical adoption yet, but formulators sourcing raw materials now should build supplier relationships capable of supporting this chemistry when development timelines converge.














