
A stonemason or countertop fabricator who spends years around respirable dust — and never develops symptoms — can still be carrying silicotic nodules quietly consolidating in lung tissue long before a chest X-ray flags anything. By the time breathlessness forces a clinic visit, the fibrosis is irreversible, the worker’s compensation claim is running toward $250,000–$500,000, and the liability question circles back to every employer in that worker’s chain. Meanwhile, in a completely different context, silicon as orthosilicic acid in food and water is circulating through the same human body contributing to bone mineral density, and silicone polymers derived from the same silicon chemistry are contacting food, drug products, and implanted devices under tightly regulated conditions. The hazard and the utility share an element — the difference is form, particle size, route of exposure, and dose.
Silicon enters the body through inhalation, ingestion, and direct tissue contact, with profoundly different outcomes depending on chemical form. Crystalline silica dust inhaled occupationally causes irreversible lung fibrosis (silicosis) and is IARC Group 1 carcinogenic. Dietary orthosilicic acid supports bone density. Medical-grade silicone polymers are biologically inert under regulatory controls.
What makes silicon uniquely difficult to communicate is that its name covers an enormous range of chemistry — from a jagged crystalline mineral lattice that destroys macrophages on contact, to a dietary trace element absorbed in the small intestine, to a cross-linked elastomer that has been implanted in the human body for decades. Each form obeys completely different biological logic. Understanding which form you are dealing with, at what dose and by what route, is not a precautionary nicety — it is the difference between managing a recognized occupational carcinogen and administering a pharmaceutical excipient considered safe enough to put inside a syringe.

Silicon as a Trace Nutrient: What Peer-Reviewed Physiology Says About Dietary Intake and Biological Roles
The human body contains roughly 1–2 grams of silicon at any given time, distributed predominantly in connective tissue, bone matrix, skin, and the aorta — concentrations that rise and fall with dietary intake and age. That makes silicon one of the more abundant trace elements in biology, yet it remains underexamined compared to iron, zinc, or magnesium. The reason is partly historical and partly analytical: silicon is difficult to measure without contamination artifacts, and its biological roles are mechanistically subtle rather than acutely dramatic.
Orthosilicic Acid: The Form That Actually Gets Absorbed
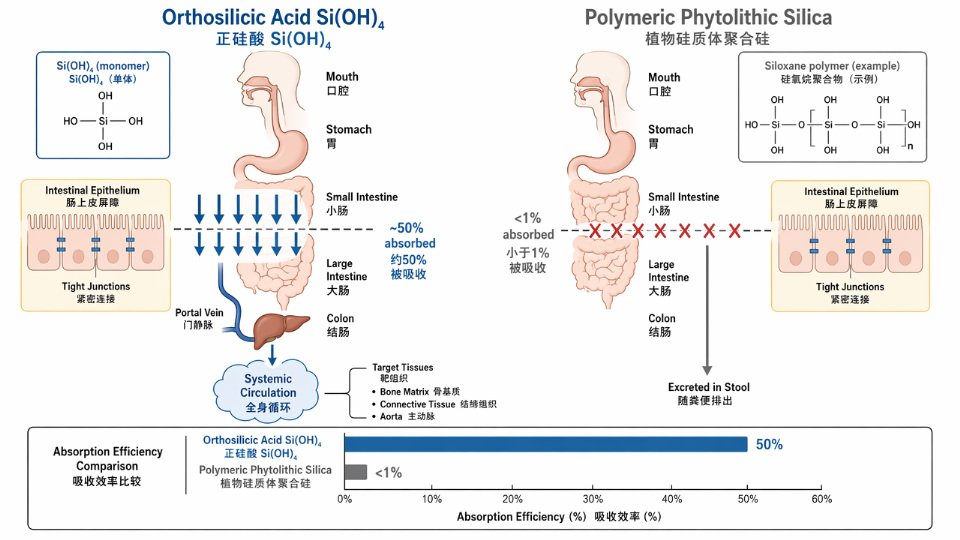
Not all silicon is biologically equivalent. The dominant bioavailable form in the gastrointestinal tract is orthosilicic acid — Si(OH)₄, a mononuclear species present in dilute aqueous solution at physiological pH. From food sources and drinking water, absorption efficiency for orthosilicic acid is approximately 50%, meaning it crosses the intestinal epithelium and enters portal circulation efficiently. The picture changes entirely for polymeric silica, including the phytolithic silica found in rice husks, cereal bran, and plant cell walls: absorption from these sources drops below 1%. The polymer cannot be broken down by human digestive enzymes, so most of it passes through.
This distinction carries real weight for anyone writing a biocompatibility data package. A formulator defending a silicone-based dietary supplement or a pharmaceutical excipient that releases orthosilicic acid needs to account for high GI uptake and systemic distribution. A food engineer evaluating rice-hull-derived anti-caking silica for a bulk powder application can reasonably expect negligible systemic absorption — but should confirm the particle characterization, because particle size and surface chemistry shift that calculation.
Typical dietary silicon intake in Western populations runs 20–50 mg Si/day, drawn primarily from grains, green vegetables, and drinking water. Asian diets, particularly where rice and millet form the staple carbohydrate, can reach around 70 mg/day, though a substantial portion arrives as poorly absorbed phytolithic silica. Drinking water contributes a meaningful fraction in high-silica geological regions: WHO data indicate typical dissolved silicon concentrations of 5–25 mg/L as SiO₂, with some groundwater sources exceeding that range.
Silicon’s Role in Bone Matrix and Connective Tissue
Silicon’s most clearly established biological function is in the structural development of connective tissue. At the cellular level, orthosilicic acid stimulates prolyl hydroxylase activity — the enzyme responsible for hydroxylating proline residues in pro-collagen chains, a mandatory step in the formation of stable collagen triple helices. Without that hydroxylation, the collagen molecule cannot fold correctly and cross-link into load-bearing fibril networks. Silicon also promotes glycosaminoglycan synthesis, supporting the proteoglycan matrix that gives cartilage its compressive resilience.
Animal models are the clearest evidence base here. Silicon-deficient chicks and rats develop abnormal bone morphology — thinner cortices, disrupted growth plates, reduced collagen content — that reverses on silicon repletion. The effect is particularly pronounced during rapid skeletal growth, which is consistent with the high silicon concentrations found in young, actively mineralizing bone and in the mitochondria of osteoblasts.
Higher dietary silicon intake is associated with greater cortical bone mineral density in premenopausal womenTrue
Jugdaohsingh et al. (2004) in the American Journal of Clinical Nutrition reported a statistically significant positive association between silicon intake and cortical bone mineral density in premenopausal women in the Framingham Offspring Cohort, after adjustment for confounders including calcium and estrogen status. The association was not significant in older postmenopausal women, suggesting an estrogen-dependent interaction.
Epidemiological Evidence and Intake Benchmarks
The Jugdaohsingh et al. (2004) Framingham Offspring Cohort analysis remains the most-cited human dataset. In premenopausal women, silicon intake in the highest quartile was associated with meaningfully higher cortical bone mineral density at the hip and spine compared to the lowest quartile — an association that persisted after adjustment for calcium intake, physical activity, and hormone status. The same association was weak or absent in postmenopausal women, pointing toward an estrogen-dependent mechanism that amplifies silicon’s osteogenic signaling.
In a typical regulatory submission for a silicone-containing food-contact material or a drug delivery excipient, this epidemiological picture is exactly what a toxicologist reaches for when building the biological plausibility argument. The baseline establishes that silicon — specifically as orthosilicic acid — is a normal constituent of human physiology, not a foreign chemical entity, which shifts the burden of evidence for harm substantially.
Quick verdict: For biocompatibility or safety data packages, the chemical form of silicon matters more than the total silicon content — orthosilicic acid and polymeric silica have absorption efficiencies roughly 50× apart, and regulators increasingly expect that distinction to be documented.
This physiological baseline is not academic background-filling. It defines the reference point against which occupational inhalation exposure, implantable device leachables, and industrial product safety assessments are judged. The following sections cover where that baseline is breached — and at what cost.
Crystalline Silica Inhalation and Silicosis: The Occupational Hazard That Kills — Mechanisms, Dose, and Latency
Silicosis does not announce itself. A worker who spent a decade cutting engineered stone countertops, grinding concrete, or dry-mixing silica flour in an abrasives plant may feel nothing abnormal for years — and then present with irreversible, progressive pulmonary fibrosis that no intervention can reverse. That latency is precisely what makes crystalline silica the most consequential occupational respiratory hazard associated with silicon-containing materials. Understanding the mechanism, the dose-response relationship, and the differences between crystalline and amorphous silica forms is not academic: it is the basis on which EHS programs are designed, supplier audits are scoped, and procurement decisions about silica-containing raw materials are made.
Why Crystalline Form Is the Critical Variable
Silicon dioxide (SiO₂) exists in both amorphous and crystalline polymorphs, and the distinction is not subtle — it is pathologically decisive. Crystalline silica, primarily in the quartz form (with cristobalite and tridymite as higher-temperature polymorphs of greater potency), is classified by IARC as a Group 1 carcinogen when inhaled in occupational settings — a classification based on sufficient evidence of lung cancer in humans, not merely animal data. The IARC Monograph Vol. 68 (1997), reaffirmed in 2012, draws that boundary explicitly at occupational inhalation; ingestion and dermal contact are not the concern here.
Amorphous silica — including fumed silica (pyrogenic), precipitated silica, and diatomaceous earth — occupies a genuinely different hazard category. It does not carry the same IARC classification, and current evidence does not support the same fibrogenic and carcinogenic potency. That said, its hazard profile is not zero: high-surface-area fumed silica grades (BET surface area commonly 200–400 m²/g) present nuisance dust hazards, and poorly crystalline or partially crystalline diatomaceous earth can contain residual quartz fractions that do warrant crystalline silica controls. “Amorphous means safe” is an operationally dangerous shortcut.
Amorphous fumed silica carries the same carcinogenic classification as crystalline quartz under IARCFalse
IARC Group 1 classification applies specifically to crystalline silica (quartz, cristobalite) inhaled in occupational settings. Amorphous silica, including fumed and precipitated grades, is not classified as a Group 1 carcinogen, though high-dust exposures still require engineering controls and health surveillance.
The Pathophysiology: How Silica Destroys Lung Architecture
The mechanism is not simple chemical toxicity — it is a self-amplifying immune cascade. Respirable particles (aerodynamic diameter Operational warning — the “we’ve always done it this way” trap: Engineering controls for crystalline silica are not a one-time installation. Local exhaust ventilation hoods drift out of position, wet suppression lines get bypassed to save cycle time, and enclosed cab positive-pressure systems lose integrity as filter maintenance lapses. What began as an adequate control becomes a documentation liability — while exposure levels creep upward over months. A supplier who cannot produce recent personal air monitoring data (not area monitoring alone) against the ACGIH TLV has almost certainly not verified that controls are performing at the worker’s breathing zone.
Quick verdict: If a supplier’s dust control program references only OSHA PEL compliance and offers no personal air monitoring data at the ACGIH TLV threshold, treat that as an open audit finding — not a pass.
How Organosilicon Compounds (Silanes, Siloxanes, Silicone Polymers) Interact With Human Biology: Biocompatibility Data That Procurement Teams Must Review
Not all silicon-based materials carry the same biological profile — and treating them as interchangeable in your SDS review process is one of the quieter compliance risks in organosilicon procurement. The chemistry that makes this family commercially versatile (tunable backbone, variable molecular weight, reactive leaving groups) is exactly what creates divergent toxicological behavior across compound classes. Procurement teams that evaluate an incoming siloxane shipment against PDMS biocompatibility data are not just wrong — they may be unknowingly accepting materials with REACH SVHC status.

Low-Molecular-Weight Cyclic Siloxanes: D4, D5, and the Regulatory Divide
Cyclic siloxanes in the D4–D6 range are low-viscosity, lipophilic, and volatile enough to cross dermal and respiratory barriers at measurable rates under occupational exposure conditions. D4 (octamethylcyclotetrasiloxane) is classified as a CMR Category 1B reproductive toxicant under REACH and sits on the SVHC candidate list as of 2018 — a designation that triggers downstream supply chain obligations including Article 33 notification duties. D5 (decamethylcyclopentasiloxane) carries an EU restriction to ≤0.1% in wash-off cosmetic products under Regulation (EU) 2018/1513 and remains under active environmental and toxicological scrutiny for bioaccumulation potential.
The biological concern with this class is systemic distribution. Animal studies have detected D4 in adipose tissue and blood following repeated inhalation exposure, consistent with its octanol-water partition coefficient. The clinical significance at low environmental doses in humans remains debated, but regulators have applied the precautionary standard rather than waiting for human epidemiological confirmation — which is the correct posture when a reproductive hazard flag is already in place.
Procurement watch-point: silicone-based personal care raw materials, release coatings, and solvent-carrier systems frequently contain residual cyclic siloxanes as process byproducts of PDMS manufacture. Incoming raw material specifications should include cyclic siloxane content limits, and SDS Section 3 should be reviewed against the REACH SVHC candidate list at each shipment, not once at supplier qualification.
Operational warning — cyclic siloxane carry-through: Residual D4/D5 levels in nominally “PDMS” products are rarely zero. A supplier’s technical datasheet may list the primary polymer correctly while the cyclic fraction appears only under GC trace impurity data or not at all. Request analytical certificates with cyclic content quantification as a contract condition, not a courtesy item.
High-Molecular-Weight PDMS: The Biocompatibility Benchmark
Polydimethylsiloxane at high molecular weight (viscosities roughly 1,000 cSt and above) represents the most extensively characterized organosilicon material in regulatory biology. Its vapor pressure is negligible, dermal absorption through intact skin is minimal, and it shows no genotoxic activity in standard Ames test or mammalian cell assays. The FDA has approved PDMS as a food-contact defoamer at ≤10 ppm under 21 CFR 173.340 and for rubber articles in food-contact service under 21 CFR 177.2600. Simethicone — activated, defoaming PDMS — carries USP/NF and EP monograph status and is administered orally as a pharmaceutical active.
For implantable-grade silicone fluid, the endotoxin limit is Unmanaged silica exposure liability compounds silently. Workers’ compensation claims for silicosis average $250,000–$500,000 per case in US occupational disease data. A single cluster of cases at one facility — not uncommon when dust controls have been drifting for years without monitoring — can generate aggregate liability that dwarfs the entire capital cost of proper LEV engineering and supplier qualification. The “temporary becomes permanent” failure mode applies here: a dust suppression system bypassed during a maintenance window and never recommissioned, or a LEV fan belt that was replaced with an undersized substitute and never re-validated.
Supplier Audit Checklist: What to Request and What Absence Signals
For procurement officers qualifying a silicon compound supplier — particularly for fumed silica, chlorosilanes, or reactive silane intermediates — the following audit criteria represent a minimum defensible standard:
| Audit Criterion | Evidence to Request | Pass Indicator | Consequence If Absent |
|---|---|---|---|
| Air monitoring records | Personal sampling results, last 12 months, by job task | Results below action level (25 µg/m³); documented sampling with NIOSH 7500/7602 | Unknown exposure profile; regulatory violation risk; liability transfer to buyer |
| LEV system validation | Inspection and commissioning logs; airflow velocity records at capture points | Documented face velocity or capture velocity meeting design spec; annual re-validation | Dust controls may be installed but ineffective; paper compliance only |
| PPE specification log | Written respiratory protection program; fit-test records; cartridge type specified | Correct cartridge (P100 or acid-gas/P100 combination for silane handling) documented per task | Workers may be wearing inadequately specified respirators |
| Medical surveillance register | PLHCP written opinions; ILO chest X-ray classification log; spirometry trend data | Current enrollment list; no overdue periodic examinations | OSHA violation; undetected early silicosis; increased legal exposure |
| Emergency response plan | Written spill response protocol; chlorosilane or reactive silane-specific procedures | Site-specific, not generic; includes acid gas release scenario | Inadequate response to chlorosilane hydrolysis events; HCl exposure risk |
| SDS currency | Supplier SDS date-stamp for each product in use | Issued or reviewed within 3 years; GHS-compliant; hazard sections 8 and 11 complete | Outdated exposure limits cited; incorrect first-aid protocols; regulatory non-compliance |
For chlorosilane and volatile silane handlers specifically, emergency eyewash and safety shower stations must meet ANSI Z358.1-2014: reachable within 10 seconds from the point of potential exposure, delivering tepid water (16–38°C) for a minimum 15-minute flush. Acid-gas cartridge respirators (with P100 particulate combination) are the specification baseline for volatile silane work — this is not a suggestion to weigh against cost, it is the engineering control minimum.
There is no validated biological biomarker for occupational crystalline silica exposure suitable for individual monitoringTrue
While urinary silicon (Si-U) shows population-level correlation with airborne silica exposure in research settings, analytical variability and dietary silicon interference (20–50 mg Si/day baseline) prevent its standardization as an individual BEI. ACGIH does not list a BEI for respirable crystalline silica. Air monitoring remains the primary quantitative tool.
A supplier who cannot produce 12 months of personal air sampling data, LEV validation records, and a current medical surveillance register is not a compliance gap to manage — it is a liability you are absorbing into your supply chain.
Silicon in Food Contact, Cosmetics, and Consumer Products: Regulatory Clearances, Extractables Limits, and What Your Formulation Buyers Need to Verify
The regulatory landscape for silicone in consumer-facing applications is deceptively fragmented. A raw material that carries an FDA approval number does not automatically make a finished article compliant — and that gap between ingredient clearance and finished-product compliance is where formulation buyers get caught. Understanding where the jurisdictional lines actually fall is the difference between a smooth market-entry dossier and a costly reformulation six months before launch.

FDA 21 CFR Food-Contact Clearances: What the Approval Number Actually Covers
Under 21 CFR 173.340, PDMS (polydimethylsiloxane) is approved as a defoaming agent in food processing at a carry-over limit of ≤10 ppm in the finished food. That approval is use-specific: it covers the functional additive in processing, not the silicone elastomer lining your baking pan. Food-contact elastomers — gaskets, tubing, bakeware — fall under 21 CFR 177.2600, which governs rubber articles intended for repeated food contact, with specific migration restrictions that depend on food type and contact temperature.
The operational trap is assuming that buying a “food-grade silicone” raw material is sufficient. It is not. Compliance belongs to the finished article, and specific migration limits apply per contact conditions. Buyers must request a finished-article declaration of compliance, not just a raw material technical data sheet. In a typical food-processing plant where silicone gaskets are sourced from multiple tier-two vendors, this verification step is routinely skipped at the procurement stage and only surfaces during an FDA audit.
EU Food Contact: Why Silicones Fall Outside Regulation (EC) No 10/2011
This surprises many procurement teams: the EU’s main food-contact plastics regulation, (EC) No 10/2011, does not cover silicones at all. Silicone food-contact materials are currently governed by national measures — primarily Germany’s BfR Recommendation XV, which specifies an overall migration limit of ≤10 mg/dm² and sets individual migration limits for volatile cyclic siloxanes D3 through D6. The Council of Europe’s ResAP(2004)5 provides a harmonizing framework, but it carries no binding regulatory force across member states in the way that (EC) No 10/2011 does for plastics.
For any silicone food-contact product being sold into EU markets, the practical standard to demonstrate compliance against is BfR XV. Suppliers should be able to provide migration test data generated per EN 1186 or equivalent methodology, at relevant contact temperatures. If a supplier cannot produce this on request, that is an audit flag.
Cosmetics: The D5 Restriction and What Dimethicone Formulators Need to Know
Under EU Cosmetics Regulation 1223/2009, cyclopentasiloxane (D5) is restricted to ≤0.1% in wash-off cosmetic products (Regulation (EU) 2018/1513, effective February 2020), on the basis of environmental persistence rather than direct human toxicity. D4 carries REACH SVHC status as a CMR 1B reproductive toxicant. Neither restriction applies to dimethicone (PDMS), which remains unrestricted and is the standard replacement for formulators moving away from volatile cyclics.
The formulation consequence matters: D5 and dimethicone are not functionally interchangeable without revalidating sensory profile, spreadability, and compatibility. Buyers switching from D5 to a linear PDMS fluid should request viscosity-matched grades (typically in the 1–50 cSt range for rinse-off feel) and confirm volatile content by loss-on-heating per ASTM D2369, since residual volatiles in a nominally “non-volatile” silicone can still trigger migration concerns in leave-on formulations.
Dimethicone (PDMS) is banned in EU cosmetics alongside D5 and D4False
Only cyclopentasiloxane (D5) is restricted in wash-off products at ≤0.1%, and D4 is listed as SVHC under REACH. Dimethicone remains permitted without restriction under EU Cosmetics Regulation 1223/2009.
Pharmaceutical Excipients and Injectable-Grade Silicone: The Endotoxin Requirement
Simethicone — activated PDMS with added silicon dioxide — is monographed in both USP/NF and the European Pharmacopoeia for use as an antifoaming agent in oral formulations. Injectable applications are a different category entirely. Silicone oil used for syringe barrel lubrication requires endotoxin testing by LAL assay, with a limit of Watch for this procurement gap: A supplier’s pharmaceutical-grade designation typically confirms purity and viscosity specifications — it does not automatically include an E&L extractables profile. Request it separately, especially for any silicone in direct or near-direct contact with drug product.
Regulatory Clearance Quick-Reference: What to Request at the Purchase Order Stage
| Silicone Product Type | Applicable Regulation / Standard | Key Limit or Specification | Verification Document to Request |
|---|---|---|---|
| Food processing anti-foaming agent (PDMS) | FDA 21 CFR 173.340 | ≤10 ppm carry-over in finished food | FDA clearance letter; processing use statement on CoA |
| Food-contact elastomer (gaskets, tubing, bakeware) | FDA 21 CFR 177.2600 / BfR Recommendation XV | Overall migration ≤10 mg/dm²; D3–D6 limits | Finished-article declaration of compliance; migration test report |
| EU food-contact silicone article | Council of Europe ResAP(2004)5 / BfR XV | Overall migration ≤10 mg/dm²; volatile siloxane limits | BfR XV compliance declaration; EN 1186 migration data |
| Cosmetic emollient (dimethicone, leave-on) | EU Cosmetics Reg. 1223/2009 | No concentration restriction; volatile content relevant | CoA with viscosity, ASTM D2369 volatile content |
| Cosmetic rinse-off fluid (D5-replacement) | EU Reg. 2018/1513 (D5 restriction) | ≤0.1% D5 in wash-off products | Supplier certificate of D5/D4 absence; viscosity-matched grade spec |
| Pharmaceutical oral excipient (simethicone) | USP/NF, EP monograph | Meets compendial identity, purity, and performance tests | CoA referencing compendial lot testing; particle size data |
| Injectable-grade [silicone oil](https://siliconchemicals.com/silicone-oil/) (syringe lubrication) | USP/NF; ICH Q3E (E&L); EP | Endotoxin Occupational health liability is not a tail risk in silica-handling operations. It is a deferred cost with a latency period — and the deferral ends in litigation, not in a budget cycle. |
Cyclic Siloxane Contamination and the EU Cosmetics Market
EU Regulation (EU) 2018/1513 restricts cyclopentasiloxane (D5) to ≤0.1% in wash-off cosmetic products, effective February 2020. D4 carries SVHC candidate list status as a CMR 1B reproductive toxicant under REACH. A personal care manufacturer purchasing cosmetic-grade dimethicone without verified D4/D5 content data — relying on a generic grade specification rather than a product-specific GC analysis — faces EU market withdrawal if finished-product testing reveals exceedance.
Testing and reformulation cost per affected SKU runs $50,000–$200,000, depending on formula complexity, clinical retesting requirements, and SKU count. In a typical mid-size personal care operation running 15–30 SKUs from a shared silicone base, a single non-compliant raw material batch can trigger a portfolio-wide review. The procurement control point is straightforward: require a batch-specific GC report for D4 and D5 content at goods receipt, not a blanket CoA noting “compliant with EU regulations” without quantitative data.
A certificate of conformity guarantees EU food-contact or cosmetics complianceFalse
A CoA confirms the supplier's own specification is met, but EU food-contact compliance under ResAP(2004)5 and cosmetics compliance under EU 2018/1513 require specific migration testing or quantitative analytical data against the relevant regulatory thresholds — not a supplier self-declaration.
Medical Device Extractables Gaps and 510(k) Delay
ICH Q3E (draft 2023) and ISO 10993-1:2018 now require structured extractables and leachables characterization for silicone components in drug-contact and implantable medical devices. An FDA 483 observation citing inadequate extractables data for a silicone tubing component — a finding increasingly common as the agency tightens expectations on polymeric leachables — can delay 510(k) clearance by 6 to 18 months. At a development burn rate of $50,000–$150,000/month for a Class II device program, that is a $300,000–$1.5M overrun, attributable directly to a materials qualification gap that could have been closed during the design phase with a supplier capable of providing extraction study data and formulation transparency.
TCO Risk Scenario Table
| Risk Scenario | Probability Tier | Estimated Direct Cost Range | TCO Multiplier vs. Prevention Cost | Procurement Control Point |
|---|---|---|---|---|
| EU food-contact migration test failure and recall | Medium | €500,000–€2M | 20–80× | Supplier qualification against ResAP(2004)5 / BfR XV; migration test CoA per batch |
| Occupational silicosis claim (single case, US) | Medium–High in uncontrolled facilities | $300,000–$700,000 per case | 5–15× per case; multiplies with workforce exposure | Air monitoring records, PEL compliance, engineering controls audit |
| EU cosmetics market withdrawal (D4/D5 exceedance) | Medium for formulators without batch GC data | $50,000–$200,000 per SKU | 10–40× | Batch-specific GC report for cyclic siloxanes at goods receipt |
| FDA 510(k) delay from silicone extractables gap | Medium in early-stage device programs | $300,000–$1.5M per program | 15–75× | Supplier extractables data package; ISO 10993-1 material qualification at design input stage |
| Batch rejection from viscosity or purity drift | High for unvalidated commodity sources | $20,000–$150,000 per affected production run | 5–30× | Incoming QC against viscosity spec, GC purity, and CoA cross-check |
Quick verdict: The cost of a qualified, documentation-capable silicon compound supplier is almost always less than 5% of a single downstream compliance failure — making supplier qualification the highest-ROI line item in silicon compound procurement.
What a TCO-Competent Supplier Qualification Looks Like
The checklist that collapses this analysis into a purchasing workflow covers: unit price and freight lead time (necessary but not sufficient); CoA completeness against the relevant regulatory standard; regulatory documentation package coverage for REACH, FDA 21 CFR, and applicable GB standards; technical support availability for formulation and compliance questions; minimum order quantity flexibility against production variability; supply continuity strategy including dual-source risk disclosure; and third-party quality audit history.
An integrated supply chain — from silicone monomer through to finished polymer, with in-house GC, XRD, FTIR, and viscometry capability — addresses most of these checklist items structurally. Batch-to-batch specification consistency, backed by instrument-verified QC rather than vendor self-attestation, converts the TCO risk scenarios above from probable line items into managed and documented non-events. That is not a premium. That is the actual cost of qualified industrial sourcing.
Frequently Asked Questions: Shop-Floor and Procurement-Desk Questions About Silicon and Human Health

Is silicone grease safe to use bare-handed on food processing equipment?
PDMS-based silicone grease carries FDA approval for incidental food contact under 21 CFR 178.3570, but that approval covers the silicone fraction only. The thickener determines the rest of the safety profile. A lithium-soap-thickened silicone grease carries a different hazard footprint than a PTFE-thickened version, and some formulations include corrosion inhibitors or antioxidants with their own exposure limits. The practical rule: pull the full SDS and the Certificate of Analysis, confirm every ingredient against your food-safety program, and verify the grade is specifically designated for food-contact or H1 classification under NSF International. Bare-hand contact with any industrial lubricant during a full shift is worth reviewing regardless — skin hydration loss and occlusion are real even when acute toxicity is low.
My workers handle fumed silica daily — should I be worried about silicosis?
Silicosis is caused by crystalline silica. Fumed silica is amorphous — structurally disordered at the atomic level — and does not carry the same pathological mechanism. That distinction matters enormously for regulatory classification and medical surveillance design. However, NIOSH recommends precautionary engineering controls for nano-amorphous silica given the 7–40 nm primary particle size and the unresolved long-term inhalation data. In practice: maintain respirable dust concentrations below 1 mg/m³ as a conservative benchmark, require closed-transfer or contained-dispensing systems for high-throughput operations, and demand an XRD crystallinity certificate from your supplier on each production lot. Amorphous does not mean inert — it means the regulatory floor is lower, not that the exposure can be ignored.
In a typical compounding operation running fumed silica at 10–15% loading into silicone elastomer, open bag-tipping into a mixer without local exhaust ventilation routinely pushes peak respirable dust levels well above the 1 mg/m³ benchmark during the pour cycle alone. The fix is a contained tipping station with ducted extraction, not a P100 respirator worn inconsistently.
We buy cyclopentasiloxane (D5) for a hair care product — is it still allowed in the EU?
D5 is restricted to ≤0.1% in wash-off cosmetic products under EU Regulation 2018/1513, effective February 2020. If your formulation exceeds that threshold in a rinse-off product sold into the EU, it is non-compliant — full stop. Suppliers should be reporting D5 content on CoA documentation, and if yours cannot, that is itself a quality-system gap. The practical pivot for affected formulations is low-cyclic PDMS fluids (linear dimethicone grades) or appropriate volatile alternatives, but performance equivalence needs bench validation before reformulation sign-off. Leave-on products currently face a separate regulatory track; monitor the EU Commission’s ongoing CMR assessments for D4 and D6 as the restriction framework continues to develop.
D5 (cyclopentasiloxane) is completely banned from all cosmetic products in the EUFalse
The EU restriction under Regulation 2018/1513 applies specifically to wash-off (rinse-off) cosmetics at concentrations above 0.1%. Leave-on products are subject to ongoing review but were not covered by the 2020 restriction.
How do I know if a silicone polymer supplier’s product is suitable for medical device tubing?
Require ISO 10993-1:2018 biocompatibility test reports, USP Class VI certification, and a complete extractables and leachables (E&L) data package — the ICH Q3E framework is the current reference for drug-contact applications. At minimum for a Class II device with prolonged skin or mucosal contact, you need cytotoxicity data (ISO 10993-5) and intracutaneous reactivity results (ISO 10993-10). Sensitization testing (ISO 10993-10 GPMT or LLNA protocol) and systemic toxicity data complete the core package. Any supplier offering medical-grade silicone polymer without this documentation ready on request is not operating at medical-grade quality — the certification is the product at that tier.
Can silicon in drinking water actually improve bone health, or is that marketing?
The science is genuine and peer-reviewed, but the effect size is modest and context-dependent. The Framingham Offspring Cohort prospective study published in the American Journal of Clinical Nutrition (Jugdaohsingh et al., 2004) found a statistically significant positive association between dietary silicon intake and cortical bone mineral density, particularly in men and pre-menopausal women. Orthosilicic acid — the form present in water and dilute aqueous solutions — absorbs at roughly 50% efficiency from the GI tract, making it the most bioavailable dietary silicon source. The operative word is “association.” Silicon is not a substitute for calcium and vitamin D, effect sizes are small relative to those micronutrients, and causal mechanisms remain under active investigation. Any product marketing making stronger claims than the actual Framingham data supports invites regulatory scrutiny. Use the evidence accurately: it is real, it is limited, and precision matters.
What’s the real difference between ‘silicon’ and ‘silicone’ on a Safety Data Sheet?
Elemental silicon (CAS 7440-21-3) is a crystalline or amorphous metalloid semiconductor — the raw material of electronics and metallurgy. Silicone refers to a class of synthetic polysiloxane polymers built on an inorganic Si–O backbone with organic substituents (methyl, phenyl, vinyl groups) attached. They have entirely different molecular structures, hazard profiles, exposure limits, biological behaviors, and regulatory classifications. An SDS that uses the two terms interchangeably is signaling either a documentation error or a deeper quality-system problem. Both should trigger a corrective action request before the material enters your facility. This is not a pedantic terminology issue — it determines which exposure limits apply, which PPE is specified, and which regulatory registers govern the substance.
Our purchasing department wants to switch to a lower-cost silane coupling agent — what health and compliance risks should we evaluate?
Start with the leaving group. Methoxy silanes release methanol on hydrolysis (OSHA PEL 200 ppm, skin notation); acetoxy silanes release acetic acid (OSHA PEL 10 ppm ceiling, strong irritant); chlorosilanes release hydrogen chloride — corrosive, with tight exposure limits and immediate PPE implications. A lower unit price on a chlorosilane grade can translate into respiratory protection program upgrades, enhanced spill containment requirements, and stricter waste classification that collectively exceed the purchase-price saving. Beyond the hazard profile, verify functional group equivalence: switching from a methacryloxy to an amino silane to cut cost in a glass-fiber composite application will change coupling chemistry and almost certainly degrade interlaminar shear strength — performance consequences that may not surface until an in-service failure, by which point the traceability trail leads back to the substitution decision.
Operational warning: The “temporary becomes permanent” failure mode is common in silane substitutions. A purchasing switch approved as a short-term cost measure during a supply crunch gets normalized into the approved supplier list without a formal re-qualification. Months later, a QA drift in bond strength or moisture resistance gets investigated as a process problem — not a material change. Lock material substitutions to your change-control procedure before approving the purchase order, not after the problem surfaces.
How to Evaluate a Silicon Compound Supplier’s Health, Safety, and Regulatory Competency: A Procurement Qualification Framework
Choosing a silicon compound supplier on unit price alone is one of the more expensive decisions a procurement team can make — the savings disappear the first time a customs hold, a failed extractables audit, or a workplace exposure citation surfaces. Every section of this article converges on one operational conclusion: the hazard profile of silicon-containing materials is specific to form, chemistry, and processing context, and a supplier who cannot document that specificity is a liability, not a resource.
The framework below is structured in three tiers that mirror how a mature procurement audit actually runs: document review first, regulatory compliance package second, site-level evidence third. A fourth criterion — technical query response capability — is often the most diagnostic of all.

Tier 1: Baseline Documentation That Should Arrive Before a Sample Does
A current, GHS-compliant Safety Data Sheet is the floor, not the ceiling. “Current” means revised within three years and reflecting any regulatory status changes — a silicone fluid SDS that does not mention D4’s SVHC status or D5’s EU wash-off restriction, for example, tells you immediately that the supplier’s regulatory monitoring is not live. The CoA must carry specification limits with upper and lower bounds, not just typical values; a CoA showing a single viscosity figure to one significant figure cannot support incoming QC decisions and should be returned.
For silica products specifically, demand an XRD crystallinity certificate from an accredited laboratory using NIOSH 7500 methodology. Amorphous fumed silica and crystalline quartz require entirely different exposure controls — a supplier who conflates them in documentation is creating downstream EHS liability for your operation. For silicone fluids and polymers, a cyclic siloxane content declaration (D3 through D6 fractions by GC) is non-negotiable for any application touching cosmetics, food contact, or pharmaceutical processing. Operators in regulated industries routinely discover that a formulation passed early-stage review on polymer backbone chemistry alone, only to fail extractables screening because cyclic content was undisclosed at the raw-material stage.
Tier 2: Regulatory Compliance Package for Market-Specific Applications
The compliance package required depends on your downstream market, but a credible supplier should hold documentation across all three major frameworks simultaneously. For EU-destined supply, a REACH registration number (or a substantiated SVHC absence declaration with CAS-level specificity) is required for any silane imported above one tonne per year — the absence of a registration number is not a paperwork gap, it is a legal barrier to import. For food processing or pharmaceutical applications, a written 21 CFR compliance letter mapping the specific regulation (173.340 for defoamer use, 177.2600 for rubber articles) to the specific product lot is the minimum; a generic “food grade” label with no citation is not compliance evidence. Electronics-grade silicones require RoHS and WEEE declarations traceable to the product formulation. For buyers sourcing from China, GB/T standard compliance documentation provides the domestic quality anchor and also signals that the supplier is operating within the regulated tier of China’s chemicals industry rather than outside it.
Tier 3: Manufacturing Site Audit Criteria
ISO 9001 QMS certification sets the process discipline baseline but does not by itself address occupational health. The site-level evidence that distinguishes a genuinely compliant manufacturer includes: respirable dust monitoring records with analytical results referenced to the OSHA PEL of 50 µg/m³ and, ideally, the more protective ACGIH TLV of 25 µg/m³; LEV inspection logs showing documented commissioning, periodic performance verification, and corrective actions; and evidence of a medical surveillance program covering workers with potential silica exposure — chest radiography at intervals consistent with NIOSH guidance is the standard practice. A third-party environmental compliance audit conducted within the last two years closes the loop on effluent and waste stream management, which matters both for ESG reporting and for regulatory continuity risk.
In a typical evaluation of a mid-volume silane sourcing decision — annual import volume in the range of 50–200 tonnes into the EU — procurement teams that request Tier 3 documentation upfront identify disqualifying gaps in roughly 30–40% of initial candidate suppliers. The gaps rarely involve outright safety failures; they are usually incomplete dust monitoring records or a medical surveillance program that exists on paper but lacks recent examination data. Those gaps, left unaddressed, become the procurement team’s liability once the material is on-site.
Technical Query Response Capability as a Qualification Signal
This is the criterion that separates integrated manufacturers from trading intermediaries, and it costs nothing to test. Send three written questions before placing any order:
- What is the D3–D6 cyclic siloxane content (% by GC) in this PDMS fluid at the offered viscosity grade?
- What is the residual chloride content (ppm) in this silane, and what is the specification limit on the CoA?
- What is the crystallinity percentage of this fumed silica, and by what analytical method was it determined?
An inability to answer all three in writing, with data traceable to a specific lot or production specification, is disqualifying for any regulated-industry application. A supplier who can answer them immediately, with method references and lot-specific data, has demonstrated process knowledge that only exists when manufacturing and analytical capability are integrated — not when product is being re-labeled from an upstream source.
A GHS-compliant SDS alone is sufficient supplier qualification for food-contact silicone applications.False
SDS compliance covers hazard communication but does not constitute regulatory clearance for food-contact use. FDA 21 CFR compliance requires a specific, lot-traceable compliance letter citing the applicable regulation section, separate from GHS documentation.
XRD crystallinity testing is necessary to distinguish amorphous fumed silica from crystalline quartz in occupational exposure assessments.True
Amorphous silica does not carry the IARC Group 1 carcinogen classification that applies to respirable crystalline silica. XRD analysis per NIOSH 7500 is the recognized method for confirming crystalline phase content and is essential for determining which exposure control standard applies.
Supplier Qualification Scorecard
| Qualification Criterion | Documentation Type | Minimum Acceptable Standard | Weight in Score (%) | SiliconChemicals Status |
|---|---|---|---|---|
| SDS compliance | GHS-aligned SDS | Revised within 3 years; SVHC and restriction status current | 15 | Full — updated to current EU and China GHS editions |
| CoA completeness | Lot-specific CoA | Upper and lower specification limits; ≥3 significant figures on key parameters | 15 | Full — specification limits with method references |
| Cyclic siloxane declaration | GC analysis report | D3–D6 fractions declared by % for all PDMS fluids and polymers | 12 | Full — lot-level GC data available on request |
| Crystallinity certificate | XRD (NIOSH 7500) | Accredited lab; crystallinity % reported per lot for silica products | 10 | Full — third-party accredited XRD per shipment |
| REACH / FDA documentation | Registration number or CFR compliance letter | REACH reg. no. for EU imports >1 t/yr; 21 CFR letter for food/pharma | 15 | Full — REACH registered; 21 CFR letters by product grade |
| ISO 9001 certification | Third-party audit certificate | Current, scope covering manufacturing and QC | 10 | Certified — scope covers monomer through specialty finishing |
| Dust monitoring records | IH air sampling records | Results vs. OSHA PEL (50 µg/m³); monitoring frequency per exposure profile | 10 | Available — periodic monitoring with LEV verification logs |
| Medical surveillance evidence | Occupational health program records | Chest radiography program for silica-exposed workers; documented intervals | 8 | Active program — records available under NDA for site audits |
| Technical query response | Written, lot-traceable responses | All three standard queries answered in writing within 5 business days | 5 | Demonstrated — technical team responds with production data |
Quick verdict: Any supplier scoring below 70% on this framework — particularly with gaps in cyclic siloxane declaration, REACH documentation, or technical query response — should not be qualified for regulated-industry applications regardless of price.
As an integrated manufacturer operating from chloromethane and silicon metal through to finished specialty silicone products within China’s Zhejiang and Shandong organosilicon clusters, SiliconChemicals holds the structural advantage that makes this scorecard achievable: batch consistency, documentation completeness, and the analytical depth to answer specification questions at the production level. That vertical integration is not a marketing claim — it is the reason the documentation exists in the first place.
If your procurement team is running a supplier qualification exercise for silanes, siloxane fluids, fumed silica, or specialty silicone polymers, our technical team is available to respond to written specification queries, provide compliance documentation packages, and discuss application-specific regulatory requirements. The conversation starts with the right questions — and those questions are now in your hands.














